
Dermarolling has become one of the more talked-about at-home treatments for hair loss — but unlike most trending interventions, it has real clinical evidence behind it. The question is not whether it works, but whether you’re using it correctly and safely.
This guide covers what the evidence actually shows, how to use a derma roller at home, the critical safety rules (especially around minoxidil timing), and who should not use one.
Does Dermarolling Actually Work for Hair Loss?
Short answer: yes — particularly for androgenetic alopecia (AGA, male and female pattern hair loss) when combined with minoxidil.
A 2025 meta-analysis published in the Archives of Dermatological Research (PMC11890238) pooled 12 randomised controlled trials involving 631 patients and found that combined microneedling plus minoxidil was significantly superior to minoxidil alone (standardised mean difference: 1.32, p<0.01). This is not a marginal effect — it’s a large, consistent, replicated finding.
The foundational clinical trial remains Dhurat et al. (2013), a 100-man randomised controlled trial in androgenetic alopecia. In that study:
- 82% of the combination group (dermarolling + minoxidil) showed more than 50% improvement in hair count
- Only 4.5% of the minoxidil-only group reached the same threshold
- Mean hair count: 91.4 new hairs per square centimetre in the combination group vs 22.2 in the minoxidil-only group
A 2025 network meta-analysis published in Frontiers in Medicine further confirmed the relative efficacy advantage of minoxidil in combination with microneedling over minoxidil alone.
Important limitation: This evidence is specifically for androgenetic alopecia. Dermarolling is not an evidence-based treatment for alopecia areata — and may in fact be contraindicated in active alopecia areata patches (see contraindications below).
Solo dermarolling (without any topical treatment) does show some benefit through growth factor release, but the strongest evidence is consistently for the minoxidil combination.
How It Works: The Mechanism
Two separate mechanisms explain why dermarolling helps with hair loss:
1. Wound healing growth factor cascade
Mechanical wounding of the scalp triggers the body’s wound healing response. This releases:
- PDGF (platelet-derived growth factor) — promotes dermal papilla cell proliferation
- VEGF (vascular endothelial growth factor) — improves follicle blood supply
- KGF (keratinocyte growth factor) — stimulates keratinocyte proliferation in the follicle
These signalling molecules push follicles from telogen (resting) back into anagen (active growth) phase, effectively waking dormant follicles.
2. Topical absorption enhancement
The microchannels created by dermarolling significantly increase the penetration depth and bioavailability of topical treatments applied to the scalp. For minoxidil, this means better delivery to the follicle — which partly explains why the combination is so much more effective than either treatment alone.
Both mechanisms work together. At shallower depths (0.25–0.5mm), absorption enhancement dominates. At deeper depths (0.75–1.5mm), growth factor stimulation becomes the primary driver of efficacy.
Needle Depth Guide
Choosing the right needle depth is the most important decision you’ll make when buying a derma roller for hair loss.
| Needle depth | Primary mechanism | Recommended frequency | Notes |
|---|---|---|---|
| 0.25–0.5 mm | Absorption enhancement (topicals) | Daily to 2–3× per week | Minimal growth factor stimulation; safe for daily use; good starting point |
| 0.75–1.0 mm | Moderate growth factor stimulation + absorption | Weekly to every 2 weeks | Best balance of efficacy and safety for most home users; some discomfort normal |
| 1.5 mm | Maximum growth factor stimulation | Every 2–4 weeks | Most evidence-based depth in clinical trials; causes significant discomfort; some sources recommend professional supervision at this depth |
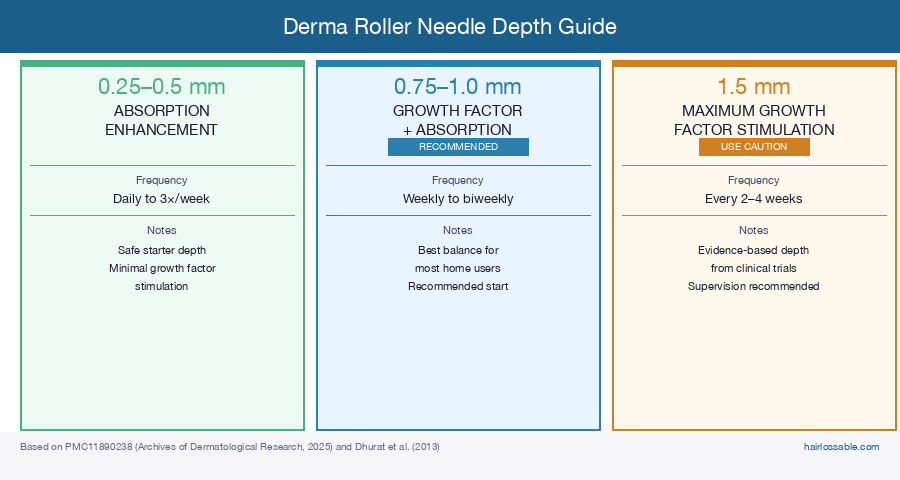 Needle depth determines which mechanism dominates. Most home users should start at 0.5–1.0 mm weekly. The 1.5 mm depth used in clinical trials produces stronger growth factor stimulation but warrants careful technique.
Needle depth determines which mechanism dominates. Most home users should start at 0.5–1.0 mm weekly. The 1.5 mm depth used in clinical trials produces stronger growth factor stimulation but warrants careful technique.
Recommendation for most home users: Start with a 0.5–1.0 mm roller used once weekly. This depth range is backed by evidence, manageable at home, and covers both the absorption-enhancement and growth-factor mechanisms.
Note on 1.5 mm: The Dhurat 2013 trial and many subsequent studies used 1.5 mm. While it is achievable at home, it causes meaningful discomfort and some practitioners recommend medical supervision at this depth. If you choose 1.5 mm, start with longer intervals (every 3–4 weeks) and consult a dermatologist if you have any scalp conditions.
⚠️ The 24-Hour Minoxidil Rule
Do not apply minoxidil immediately after dermarolling.
This is the most important safety point in this entire guide — and one of the most frequently skipped or minimised in popular content.
Here’s why it matters: dermarolling creates thousands of microchannels in the scalp, dramatically increasing the permeability of the skin barrier. This is useful for enhancing minoxidil delivery in normal use — but if you apply minoxidil while those channels are open, systemic absorption increases far beyond normal levels.
Excessive systemic absorption of topical minoxidil can cause:
- Hypotension (low blood pressure, dizziness, lightheadedness)
- Tachycardia (rapid or irregular heartbeat)
- Other systemic minoxidil side effects at elevated severity
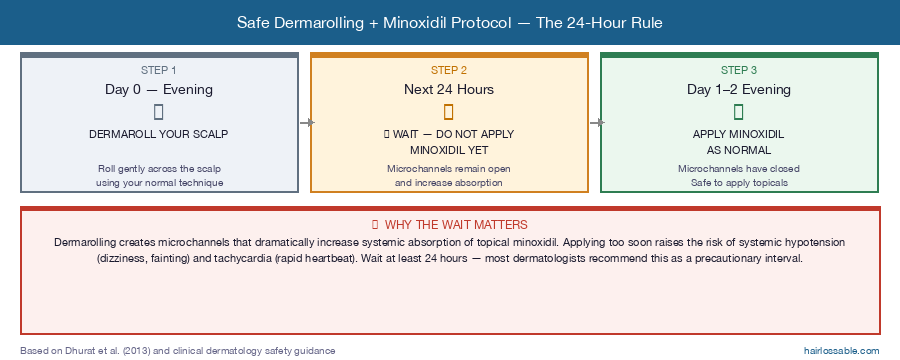 The 24-hour rule is a safety requirement, not a suggestion. Dermarolling creates microchannels that dramatically increase minoxidil absorption — applying too soon raises the risk of systemic hypotension and tachycardia.
The 24-hour rule is a safety requirement, not a suggestion. Dermarolling creates microchannels that dramatically increase minoxidil absorption — applying too soon raises the risk of systemic hypotension and tachycardia.
The safe protocol:
- Dermaroll your scalp
- Wait at least 24 hours — most dermatologists and practitioners recommend this as a precautionary interval while microchannels remain open
- Apply minoxidil as normal after the microchannels have closed
A simple pattern: roll in the evening, apply minoxidil the following evening.
This timing rule applies to other topicals too. Do not apply any topical product (minoxidil, topical finasteride, peptide serums, essential oils) to a freshly-rolled scalp within the 24-hour window.
Scalp Contraindications: Who Should Not Dermaroll
Dermarolling is not appropriate for everyone. Do not use a derma roller if you have any of the following:
- Active scalp psoriasis flare — the Koebner phenomenon means mechanical trauma can trigger new psoriatic lesions
- Seborrheic dermatitis outbreak — rolling over inflamed, flaking skin increases infection risk and worsens irritation
- Active alopecia areata patches — mechanical trauma may trigger or worsen lesions in active AA; dermarolling is not evidence-based for AA and may cause harm in active disease
- Infected scalp or open wounds/lesions — rolling over broken skin spreads bacteria and causes serious harm
- Heavily sunburned scalp — compromised skin is at higher risk of adverse reactions
- Anticoagulant medications (blood thinners) — increased bleeding risk from needle punctures; consult your doctor before use
- History of keloid scarring — risk of abnormal scar formation
If you have any of the above, consult a dermatologist before using a derma roller.
Even without formal contraindications, pause use if your scalp is acutely irritated, itchy, or inflamed from any cause, and resume only when the scalp has settled.
What Results to Expect and When
Dermarolling does not produce fast results. Understanding the realistic timeline prevents early abandonment.
Typical timeline:
- 0–8 weeks: No visible change. Underlying follicle activity is shifting but hair growth is not yet apparent.
- 12 weeks: Some people begin to notice early changes in hair density or texture. This is the minimum time point most clinical trials use for interim assessment.
- 24–52 weeks: Most studies show peak benefit in this range with consistent weekly use. The Dhurat trial assessed results at 12 weeks; longer protocols tend to show continued improvement.
What determines results:
- Consistency of protocol — irregular use substantially reduces efficacy
- Needle depth and frequency — these must match (deeper = less frequent)
- Whether you’re combining with minoxidil or another topical — combination use has far stronger evidence than rolling alone
- Severity and duration of hair loss — results in more advanced loss may be more modest
“Results are protocol-dependent, not product-dependent.” A cheap dermaroller used consistently and correctly will outperform an expensive one used sporadically or incorrectly.
Choosing a Roller and Keeping It Clean
Needle material
Titanium needles maintain their sharpness longer than stainless steel and are more resistant to bending. Stainless steel rollers are a functional option but blunt faster, and blunt needles tear skin rather than pierce cleanly.
This is not a product recommendation — both materials are widely available at various price points. The principle: sharper, undamaged needles cause cleaner punctures and heal faster.
When to replace
Replace your dermaroller every 10–15 uses. After that point, needle tips become microscopically blunt or bent even if they look intact, and the punctures they create are less clean.
Sterilisation (required before every use)
- Rinse under clean running water after use to remove any debris
- Submerge the roller head in 70% isopropyl alcohol for 5–10 minutes
- Allow to dry completely before use (wet needles on a fresh scalp can dilute or irritate)
- Store in the protective case
Never share a dermaroller. Shared rollers transmit bloodborne pathogens. Each person should have their own.
Home Dermarolling vs Clinical Microneedling: How They Compare
At-home dermarolling and professional microneedling are related but distinct procedures. Understanding the difference helps you choose the right approach.
| At-home dermarolling | Clinical microneedling | |
|---|---|---|
| Needle depth | 0.25–1.5 mm | 1.5–2.5 mm (or more) |
| Control | Manual (rolling motion) | Motorised pen (vertical stamping motion) |
| Sterility | User-sterilised | Clinical-grade sterile environment |
| Add-ons | Topical minoxidil, serums | PRP (platelet-rich plasma), growth factors |
| Frequency | Weekly to every 4 weeks | Every 4–8 weeks |
| Evidence | Strong for minoxidil combination (home-depth studies) | Strong; clinical studies often use 1.5 mm+ |
| Supervision | None | Dermatologist or trained practitioner |
| Cost | Low upfront, minimal ongoing | Higher per session |
For most people with AGA who want to add dermarolling to their routine, home use with a 0.5–1.0 mm roller plus minoxidil is a well-evidenced, accessible starting point. Clinical microneedling makes sense if you want professional oversight, PRP combination, or are not seeing adequate results from home use.
For a full comparison of the clinical procedure, see our microneedling for hair loss guide.
Frequently Asked Questions
Does a derma roller help with hair loss?
Yes, specifically for androgenetic alopecia (AGA). The evidence is strongest for dermarolling in combination with minoxidil — multiple randomised controlled trials and a 2025 meta-analysis of 12 RCTs show significantly better results than minoxidil alone. It is not evidence-based for alopecia areata.
Can I use minoxidil after dermarolling?
Not immediately. Most dermatologists and practitioners recommend waiting at least 24 hours after dermarolling before applying minoxidil. Applying minoxidil to a freshly-rolled scalp dramatically increases systemic absorption, which can cause hypotension and tachycardia. Apply minoxidil the following day, after the microchannels have closed.
What needle size should I use for hair loss?
For most home users, 0.5–1.0 mm used once weekly is the recommended range. This covers both the absorption-enhancement and growth-factor mechanisms and is manageable without professional supervision. Start at the lower end and only increase depth if tolerated well.
The Bottom Line
Dermarolling is one of the better-supported adjunct treatments for androgenetic alopecia. It is not a standalone cure, but used consistently alongside minoxidil, it has replicated RCT evidence showing meaningful improvements in hair density.
The key rules:
- Wait at least 24 hours after rolling before applying minoxidil — most dermatologists and practitioners recommend this as a precautionary interval; do not skip it
- Use an appropriate depth (0.5–1.0 mm for most people)
- Replace your roller every 10–15 uses and sterilise before every session
- Don’t use it on contraindicated scalp conditions
- Give it at least 12–24 weeks of consistent use before evaluating results
For information on prescription treatments that can be used alongside dermarolling, see our guides on oral minoxidil and the minoxidil and finasteride combination.
This article is for informational purposes only and does not constitute medical advice. Consult a dermatologist or trichologist before starting any new hair loss treatment, particularly if you have scalp conditions or take medications.
References
- PMC11890238 — Meta-analysis, Archives of Dermatological Research (2025): 12 RCTs, 631 patients; combined microneedling + minoxidil vs minoxidil alone; SMD 1.32, p<0.01.
- Dhurat R, et al. “A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study.” International Journal of Trichology (2013). 82% vs 4.5% >50% improvement; hair count 91.4 vs 22.2.
- Network meta-analysis, Frontiers in Medicine (2025): relative efficacy of minoxidil in combination with microneedling modalities.