If you’ve noticed extra hair on your pillow, in the shower drain, or wrapped around your hairbrush, the first question worth asking is: is this actually hair loss — or is it breakage?
The distinction matters more than most people realise. Hair breakage and true hair loss look similar at a glance, but they have completely different causes and completely different solutions. Treating one as if it’s the other wastes money, misses the actual problem, and — in the case of real hair loss — can delay treatment that might preserve follicles.
Here’s how to tell them apart.
The fastest way to tell: look for the bulb
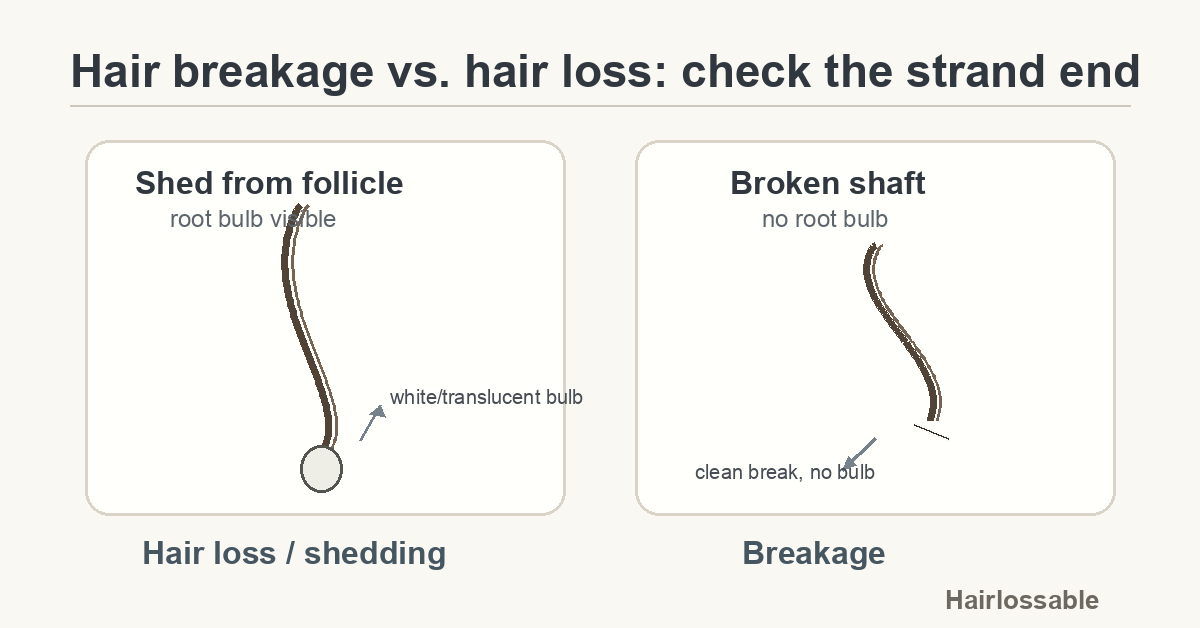
Check the root end: a white bulb means the strand fell from the follicle (hair loss). No bulb — just a clean break — means the shaft broke (breakage).
Pick up one of the fallen strands and examine the end that came from your scalp.
If it has a small white or translucent bulb: That’s the hair root. The strand shed from the follicle. The bulb may have a semi-transparent sheath attached (the inner root sheath). Losing a few bulbed strands every day is completely normal — humans naturally shed around 50–100 hairs per day as part of the regular hair growth cycle.
If there’s no bulb — just a blunt break or tapered end: The strand snapped along the shaft. This is breakage, not shedding. The follicle is still intact; you’re losing fibre length, not follicle function.
This single visual check resolves the question in most cases.
What strand length tells you
Hairs that shed from the root are usually full length, or close to it. Broken hairs tend to be short and uneven: fragments of inconsistent length, sometimes with rough or frayed ends.
If most of what you’re finding is short, varying-length pieces with no bulb, that’s almost always breakage.
How to check more carefully
Look at the strand collection as a whole. Pull a small sample from the brush or drain. Are most strands full-length with a visible bulb? That points toward shedding from the follicle. Are most strands short, varying lengths, no bulb? That points toward breakage.
The pull test (for follicular shedding). Gently clasp about 60 hairs between thumb and index finger near the scalp. Slowly draw your fingers along the shaft toward the tips. If more than 6 hairs come free with a gentle tug — and they come with bulbs — this suggests elevated shedding. A positive pull test doesn’t diagnose a cause; it confirms that shedding is above the normal daily rate. A dermatologist can perform a more standardised version.
Look at your scalp. Follicular hair loss can reduce visible density at the parting line, temples, or crown over time. Breakage, by contrast, doesn’t change follicle density — it shortens hairs but doesn’t deplete them. If your part looks wider or your scalp is becoming more visible at the hairline, that points toward genuine hair loss.
Look at the texture of the remaining hair. Breakage is almost always accompanied by other signs of damage along the shaft: frizz, dullness, split ends, rough texture when running fingers from root to tip. Hair that sheds cleanly from a healthy follicle doesn’t typically show these signs.
What causes hair breakage
Hair breakage happens along the shaft, not at the root. It’s a structural failure of the hair fibre — the follicle is intact; the strand itself has been weakened to the point where it fractures under normal stress.
Heat damage. Blow dryers, flat irons, and curling irons at high temperatures — particularly above around 230°C (450°F) — disrupt the hydrogen bonds and eventually the disulfide bonds that hold the hair’s cortex together. Repeated high-heat styling without heat protection progressively weakens the shaft.
Chemical damage. Bleaching, chemical relaxers, and perms all work by breaking and reforming the disulfide bonds in the hair cortex. Done repeatedly or without adequate recovery time, this leaves the cortex structurally compromised. Heavily processed hair — particularly at the junction between treated and new growth — is especially vulnerable to snapping under everyday tension.
Mechanical damage. Friction and physical stress cause breakage without chemistry. Rough towel-drying, dry brushing, tight elastic bands, aggressive combing on wet hair, and rough pillowcase fabric can all cause shaft fractures, especially at points of highest stress.
Extreme dryness. Chronically dry hair — from over-washing, certain detergents, or low-humidity environments — loses elasticity and becomes brittle. Brittle hair fractures under forces that healthy, well-moisturised hair absorbs.
Protein deficiency (rare). Hair is made almost entirely of keratin, a protein. Severe protein deficiency — uncommon in most contexts but possible with very restrictive diets or significant malabsorption — can weaken the shaft structure. This is distinct from follicular hair loss: it weakens the fibre, not the follicle. (In cases of extreme malnutrition, severe calorie and protein restriction can also trigger telogen effluvium — a follicular effect — in addition to shaft weakness, but this is a separate mechanism.)
What breakage is not: Hair breakage is not caused by androgenetic alopecia, telogen effluvium, hormonal conditions, thyroid dysfunction, or nutritional deficiencies affecting the follicle. Those conditions operate at the root level. Breakage is a surface problem; follicular hair loss is a root problem.
What causes true hair loss (shedding from the follicle)
When hair sheds with a bulb — especially more than usual, or without adequate regrowth — the cause is at the follicle level. The main categories:
Androgenetic alopecia (genetic hair loss). The most common form of hair loss in both men and women. Caused by genetic sensitivity to dihydrotestosterone (DHT), which gradually miniaturises susceptible follicles over years. In men, it typically presents as a receding hairline or crown thinning; in women, as widening of the central part or diffuse thinning at the crown with the hairline largely preserved. Without treatment, AGA is progressive.
→ See: Female pattern hair loss
Telogen effluvium (trigger-related shedding). After a significant physiological stressor — serious illness, surgery, major weight loss, childbirth, or high fever — a large number of follicles can simultaneously enter the resting (telogen) phase. About two to three months later, those follicles shed, producing a wave of diffuse, full-length shedding with bulbs attached. Telogen effluvium is usually self-limiting; once the underlying trigger resolves, the hair cycle typically restores itself.
→ See: Telogen effluvium
Nutritional deficiencies. Iron deficiency — particularly low ferritin — is one of the most common reversible causes of diffuse hair shedding in women. Deficiencies in vitamin D and zinc can also disrupt the hair growth cycle. These affect follicle function, not shaft integrity, and are diagnosed through blood tests rather than by examining the strands themselves.
Hormonal conditions. Thyroid dysfunction (both underactive and overactive), polycystic ovary syndrome (PCOS), and hormonal shifts during the postpartum period or menopause can all trigger hair shedding. These require medical investigation and management.
Alopecia areata. An autoimmune condition in which immune cells attack hair follicles, producing sudden, patchy hair loss. Distinct from the diffuse thinning of androgenetic alopecia and from breakage.
Medications. Certain drugs — including some chemotherapy agents, anticoagulants, antidepressants, and retinoids — can trigger hair shedding as a side effect, typically via telogen effluvium.
What to do next
If it’s breakage
The solution is addressing the physical cause of shaft damage:
- Reduce heat. Lower your styling tool temperatures; use a heat protectant; air-dry when possible.
- Space out chemical treatments. Allow adequate recovery time between bleaching, relaxing, or perming sessions; use deep conditioning treatments regularly.
- Change mechanical habits. Use a wide-tooth comb on wet hair; swap tight elastic bands for fabric scrunchies; switch to a satin or silk pillowcase; pat hair dry rather than rubbing.
- Restore moisture and structural integrity. Deep conditioning masks and bond-repair treatments (those containing ingredients that reform broken disulfide bonds) can help structurally damaged hair recover over time.
Breakage does not benefit from minoxidil, finasteride, hair loss supplements, or any treatment targeting the follicle. The follicle is not the problem.
If it’s hair loss (shedding from the root)
The appropriate response depends on the cause, which requires investigation:
- Track the pattern. Is it diffuse across the scalp, or concentrated at the hairline, crown, or part? Has it been gradual over years, or sudden and recent? Note any significant stressors, illnesses, major diet changes, or new medications in the three months before the shedding started.
- Get basic bloodwork. For unexplained diffuse shedding, a standard panel — ferritin, vitamin D, thyroid function (TSH, free T4), and a full blood count — can rule out the most common correctable causes.
- See a dermatologist or GP. Pattern hair loss and autoimmune conditions respond better to treatment when identified early. A clinician can confirm the cause through examination and, if needed, a scalp biopsy or further tests.
Can you have both at the same time?
Yes — and it’s more common than most people expect.
Someone with androgenetic alopecia who also uses frequent heat styling may be experiencing both follicular miniaturisation and shaft breakage simultaneously. The two have independent mechanisms: one originates at the follicle; the other along the shaft. They coexist without one causing the other.
If you’re finding both full-length shed hairs with bulbs and short broken fragments, you’re likely dealing with both. The approach is the same: address the breakage by modifying hair care habits, and investigate the follicular loss separately.
One useful sign: if you stop heat styling and things improve somewhat but not fully, the remaining shedding is probably follicular — worth following up on.
Summary
| Hair breakage | Hair loss | |
|---|---|---|
| Bulb at the end? | No | Yes |
| Strand length | Short, uneven fragments | Full-length or near full-length |
| Shaft texture | Frizz, split ends, dullness | Usually normal |
| Scalp visibility | Unchanged | May increase over time |
| Cause | Heat, chemicals, mechanical damage | AGA, TE, hormonal, nutritional, autoimmune |
| Fix | Change hair care habits | Investigate and treat the underlying cause |
Getting the distinction right means you’re solving the actual problem — not the wrong one.
This article is for informational purposes only and is not a substitute for professional medical advice. If you’re concerned about hair loss, speak with a dermatologist or your GP.