Medically reviewed by Dr. Ana Reyes, DO
If you’ve noticed your hairline starting to change, or you’re finding more hair than usual in the shower, you’re not imagining it — and you’re not alone. Roughly 25% of men with androgenetic alopecia (AGA) begin showing signs before age 21, according to the American Hair Loss Association. Early hair loss is more common than most people in their 20s realize.
The most common cause of hair loss in young adults is AGA — genetic pattern loss driven by sensitivity to the hormone DHT. It won’t reverse on its own. But here is the real good news: early treatment with finasteride and/or minoxidil produces significantly better outcomes than waiting. The sooner you act, the more follicular function you preserve.
Losing hair in your 20s is deeply distressing. This article is written to give you a clear, honest picture — not to minimize what you’re going through, and not to sell you anything. It covers what’s happening, whether it might not be AGA at all, what treatments actually work, and what a realistic outcome looks like.
YMYL note: Diagnosing the cause of your hair loss and starting prescription treatments such as finasteride requires assessment by a GP or dermatologist. Do not start finasteride without a medical evaluation.
Is It Normal to Lose Hair in Your 20s?
Normal shedding vs. AGA
There is a meaningful difference between normal hair cycling and progressive hair loss, and confusing the two leads people either to panic unnecessarily or to miss an early treatment window.
Normal: Losing 50–100 hairs per day is a healthy, expected part of the hair growth cycle. Hair follicles cycle continuously through three phases — anagen (active growth, lasting 2–7 years), catagen (brief transition), and telogen (resting and shedding, lasting roughly 3 months). What you see in the shower is mostly telogen hairs completing their cycle. This is not hair loss in the clinical sense.
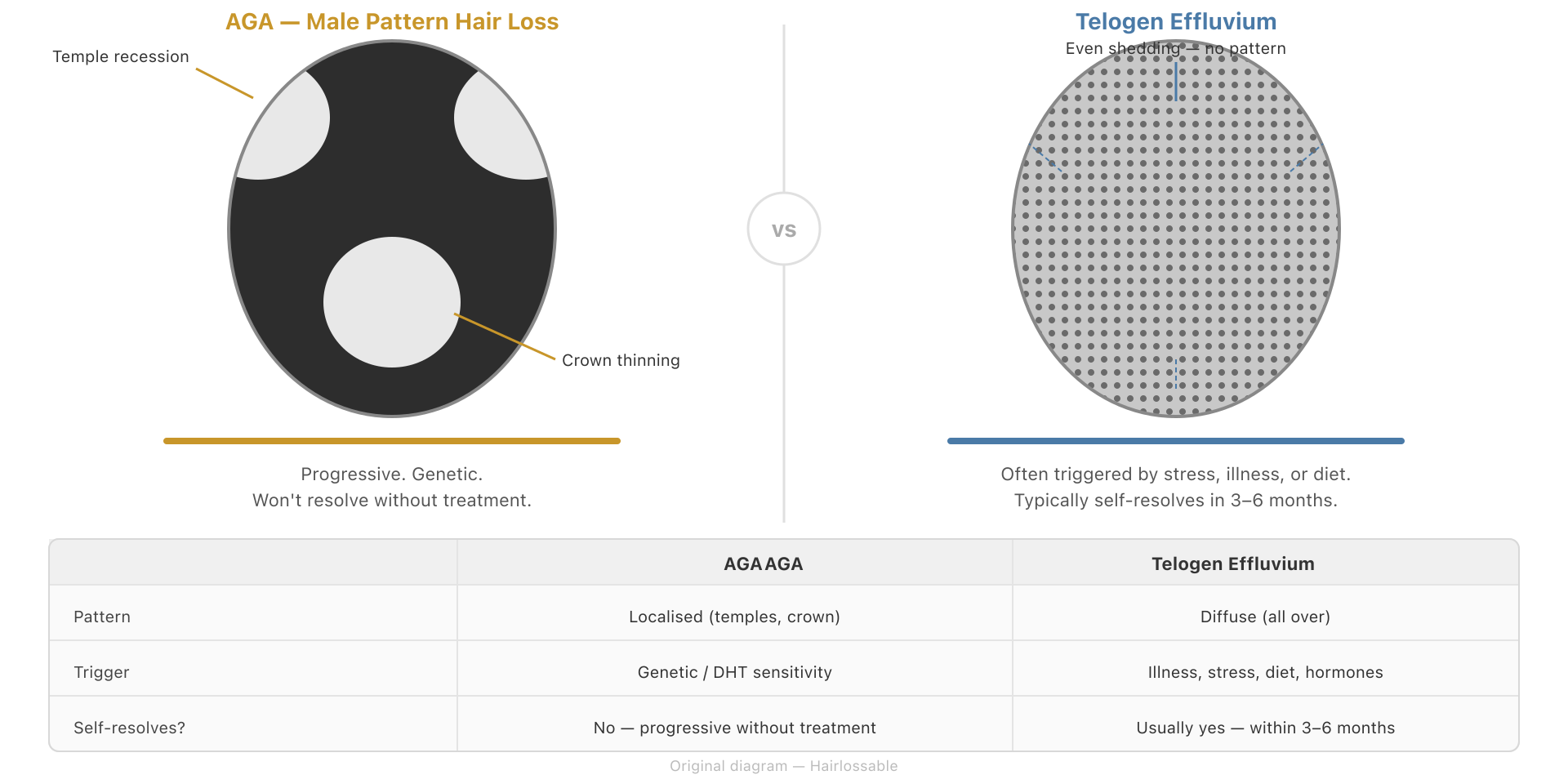
Concerning: Progressive thinning in a patterned distribution — a hairline moving back at the temples, thinning at the crown, or a widening center part in women — is a different matter. These are signs of androgenetic alopecia, not normal cycling.
The diagnostic hallmark of AGA is miniaturization: over successive growth cycles, affected follicles produce hairs that are progressively shorter, finer, and lighter in color, until the follicle eventually stops producing visible hair altogether. If the hairs you’re losing are thinner and shorter than they used to be, that matters.
How common is early AGA?
The American Hair Loss Association states that approximately 25% of men with androgenetic alopecia begin showing signs before age 21. By age 35, approximately 66% of men will have experienced some degree of AGA. By age 50, the figure rises to around 85%.
Starting early does not mean you will lose all your hair quickly. Progression rate is highly variable and influenced by genetics, the specific androgen receptor sensitivity you’ve inherited, and other factors that are not yet fully understood. Some men lose hair rapidly through their 20s; others have gradual, slow progression across decades. What is consistent is that the process does not stop or reverse on its own.
For women in their 20s: AGA is less commonly diagnosed in this decade than in men, but female pattern hair loss (FPHL) can begin in the 20s, particularly in women with polycystic ovary syndrome (PCOS) or a strong family history. We cover this in a dedicated section below.
What Causes Hair Loss in Your 20s?
Androgenetic alopecia — the most common cause
AGA is driven by a genetic sensitivity of scalp hair follicles to DHT (dihydrotestosterone). DHT is produced from testosterone by an enzyme called 5-alpha reductase. In susceptible follicles — those with androgen receptors that respond to DHT — the hormone shortens the anagen (growth) phase with each successive cycle and progressively miniaturizes the follicle.
The genetics are polygenic, meaning multiple genes are involved, and they can be inherited from either parent. The widely repeated idea that AGA only comes from your mother’s side is a myth. Your father’s hairline, your mother’s father, your maternal and paternal grandmothers — all are relevant inputs to your genetic risk.
In young men, the mechanism is identical to AGA in older men. The difference is that at 20, the follicles have had less time to miniaturize, which means there is more follicular function to preserve with early treatment. This is the core reason why acting early is advantageous.
Other causes to rule out
Before assuming AGA, it is worth considering other causes — particularly in young adults, where reversible causes are proportionally more common. Getting the diagnosis right matters because the treatments are completely different.
| Cause | Pattern | Distinguishing feature | Next step |
|---|---|---|---|
| Telogen effluvium (TE) | Diffuse all-over shedding | Triggered by a specific event 2–3 months prior: illness, surgery, high fever, rapid weight loss, major stress, or hormonal change (e.g., coming off the pill) | Often self-resolves within 6 months; see a GP if shedding exceeds 4–6 months |
| Iron deficiency | Diffuse shedding | Often accompanied by fatigue, pallor, poor concentration; confirmed by blood test | Ferritin test via GP; iron supplementation if deficient |
| Thyroid dysfunction | Diffuse shedding | May have other thyroid symptoms (fatigue, weight change, cold intolerance); confirmed by blood test | GP thyroid panel (TSH, free T4) |
| Alopecia areata | Patchy, smooth bald spots | Well-defined coin-sized patches; not a receding pattern; often sudden onset | Dermatologist referral; multiple treatment options exist |
| Traction alopecia | Loss at hairline and temples | Related to tight hairstyles — braids, ponytails, extensions | Loosen hairstyles; usually partially reversible if caught early |
Telogen effluvium is particularly worth understanding because it is common in young adults and is frequently misidentified as AGA. The defining feature is the timing: TE causes a diffuse, all-over shed that begins approximately 2–3 months after a triggering event, per well-established evidence in the clinical literature (StatPearls; Cleveland Clinic). If you can identify a stressor — an illness, a crash diet, a period of extreme stress — that preceded your hair loss by roughly 2–3 months, TE is a strong candidate. TE from a single trigger typically resolves within 6 months without treatment. AGA does not.
How to tell if it’s AGA
For men: Look for the Norwood pattern. AGA in men follows a characteristic progression: recession at the temples (corners of the hairline moving back), thinning at the vertex (crown), or both simultaneously. The pattern is more diagnostically meaningful than the amount of hair you are currently losing. If your hairline is receding rather than just changing from a juvenile to a mature hairline, that is significant.
For women: AGA in women follows the Ludwig pattern — diffuse central thinning with a widening part, but with the frontal hairline generally preserved. A receding hairline is less typical of female AGA.
Dermatoscopy — where a trichologist or dermatologist examines the scalp with a magnifying device — can assess miniaturization at the follicular level before it is visible to the naked eye. This is the most reliable confirmatory tool for AGA.
If you are uncertain: See a GP or dermatologist. Ask for blood tests covering ferritin, full blood count, and thyroid function. This rules out the reversible causes above. Do not assume AGA without a proper assessment — and do not start prescription medication without one.
What Treatments Actually Work for Early Hair Loss?
Finasteride — the most effective option for men
Finasteride 1 mg/day works by inhibiting type II 5-alpha reductase — the enzyme that converts testosterone to DHT. This reduces scalp DHT levels by approximately 64%, according to pharmacological studies (Dallob et al., Journal of Clinical Endocrinology & Metabolism, 1994; confirmed in subsequent dose-ranging studies). Less DHT at the follicle level means the miniaturization process is dramatically slowed or halted.
The clinical evidence for finasteride in AGA is substantial. In a landmark 5-year clinical trial, the vast majority of men on finasteride maintained or improved their hair density, while most men on placebo continued to lose hair (Kaufman et al., Journal of the American Academy of Dermatology, 2008; PMID 18573712). The trial data show a 93% relative reduction in the likelihood of further visible hair loss compared to placebo — meaning finasteride was dramatically more effective at protecting hair than doing nothing.
Why starting early matters: Finasteride works best as a preservation strategy. It is more effective at halting further miniaturization than at regrowing hair from follicles that have already undergone extensive fibrosis. Starting at an early Norwood stage, when the majority of follicles still retain function, gives finasteride — and you — the most to work with.
Side effects: Sexual side effects (reduced libido, erectile dysfunction, ejaculatory changes) occur in a minority of men in clinical trials and are typically reversible on discontinuation. Mood effects, including depression, have been reported. These must be weighed honestly, not dismissed.
Post-Finasteride Syndrome (PFS): A subset of men report persistent sexual, neuropsychiatric, and physical symptoms after stopping finasteride — a pattern labeled post-finasteride syndrome. The evidence here is seriously contested. The syndrome is not listed in standard product labelling as a confirmed entity, and some researchers attribute reported persistence to nocebo effects or underlying vulnerabilities that predate finasteride use. However, enough anecdotal and emerging scientific evidence exists that the medical community takes it seriously. A 2025 review by Cilio et al. in the International Journal of Impotence Research describes PFS as a “true clinical entity” warranting further study. A 2022 systematic review and meta-analysis of 34 studies found that 5-ARI use was associated with a 1.87-fold increase in PFS-like adverse effects compared to placebo — though notably, similar symptoms were also reported in placebo arms (Zhang et al., Asian Journal of Andrology, 2022; PMID 34747724). The honest summary: PFS appears real for some men, its true prevalence is unknown, and it should be disclosed and discussed with a prescribing clinician before starting finasteride. It should not be dismissed, and it should not be catastrophized.
Requires Rx: Finasteride requires a prescription in most countries. Do not start it without a GP or dermatologist assessment, including discussion of your medical history and side-effect profile.
For a deeper look at finasteride — mechanism, dosing, clinical evidence, and side effects — see our full finasteride guide.
Minoxidil — for men and women
Topical minoxidil (2% for women; 5% for men, or 5% for women in some protocols) is the only FDA-approved topical treatment for pattern hair loss. Unlike finasteride, minoxidil does not target DHT. It works through a different pathway: it is a potassium channel opener that appears to prolong the anagen (growth) phase and increase blood flow to the follicle, stimulating overall follicle activity.
Topical minoxidil is available over the counter in most markets. It is applied directly to the scalp once or twice daily. Common side effects include initial increased shedding during the first 4–8 weeks (the follicle “purge” as telogen hairs are expelled to make way for anagen hairs) and scalp irritation. Systemic side effects from topical application are uncommon but possible.
Oral minoxidil (low-dose, off-label use — typically 0.25–1.25 mg/day for women, 2.5–5 mg/day for men) is increasingly used by dermatologists, particularly for patients who do not tolerate topical application, or where systemic coverage of all scalp areas is preferred. Oral minoxidil requires a prescription. Potential cardiovascular effects mean it must be prescribed and monitored by a clinician.
Both forms must be continued indefinitely. Stopping minoxidil leads to resumed hair loss within 3–6 months as the stimulatory effect is removed.
For a detailed guide including dosing and side effects, see our oral minoxidil guide.
Combination therapy: finasteride + minoxidil
The combination of finasteride and minoxidil is more effective than either alone. These two treatments work via independent mechanisms — finasteride reduces the DHT-driven miniaturization signal; minoxidil stimulates follicle growth independently of androgen pathways — which means their benefits are additive.
A 2025 systematic review and meta-analysis of seven randomized controlled trials (N = 396 men, across relatively small individual trials) published in Frontiers in Medicine confirmed that topical minoxidil-finasteride combination produced clinically meaningful improvements in hair density, hair diameter, and global photographic assessment compared to minoxidil monotherapy, across studies from multiple countries. The established conclusion across the literature is that combination outperforms either drug alone.
For young adults starting early, combination therapy may be the most efficient long-term strategy — two complementary mechanisms working in parallel from the beginning. That said, it also doubles the potential for side effects and requires GP supervision for the finasteride component.
See our full finasteride + minoxidil combination guide.

The case for early intervention
Follicle miniaturization is not merely slow — it is progressive and, once follicles reach fibrosis, largely irreversible without surgical intervention. Early-stage miniaturized follicles respond meaningfully to finasteride and minoxidil. Late-stage follicles that have lost most of their structural integrity do not.
The “wait and see” approach is biologically counterproductive in AGA. There is no natural process that halts or reverses AGA without treatment. Every month of untreated progression is follicular function that cannot be recovered with medication alone.
The Norwood Scale — Understanding Your Pattern
The Norwood-Hamilton scale is the standard classification system for male pattern hair loss. It describes seven stages of progression:
- Norwood I: No significant recession; the juvenile hairline is intact. Not typically considered AGA.
- Norwood II: A slight recession at the temples, forming a triangular pattern. Mild early AGA.
- Norwood III: More pronounced recession at the temples. Two variants exist: Stage IIIa, where frontal recession is the dominant feature, and Stage IIIv (vertex), where crown thinning is the primary presentation. This is the stage at which most dermatologists recommend beginning treatment.
- Norwood IV: Significant recession anteriorly and thinning at the crown, with a band of hair separating the two areas.
- Norwood V: The anterior recession and crown thinning become more connected; the band separating them narrows.
- Norwood VI: The anterior and vertex areas merge. Significant hair loss across the top of the scalp.
- Norwood VII: Only a horseshoe-shaped band of hair remains at the sides and back of the scalp.
Practical guidance by stage:
- Norwood I–II: Hair is at early risk. This is the optimal window to start medical treatment — finasteride preserves what is there; there is the most to preserve.
- Norwood III–IV: Medical treatment is strongly recommended to slow progression. Significant regrowth is possible in areas with residual follicular activity.
- Norwood V–VII: Medical treatment can slow further loss but the scope for regrowth is reduced. Hair transplant surgery becomes a realistic part of the long-term plan for some men at these stages.
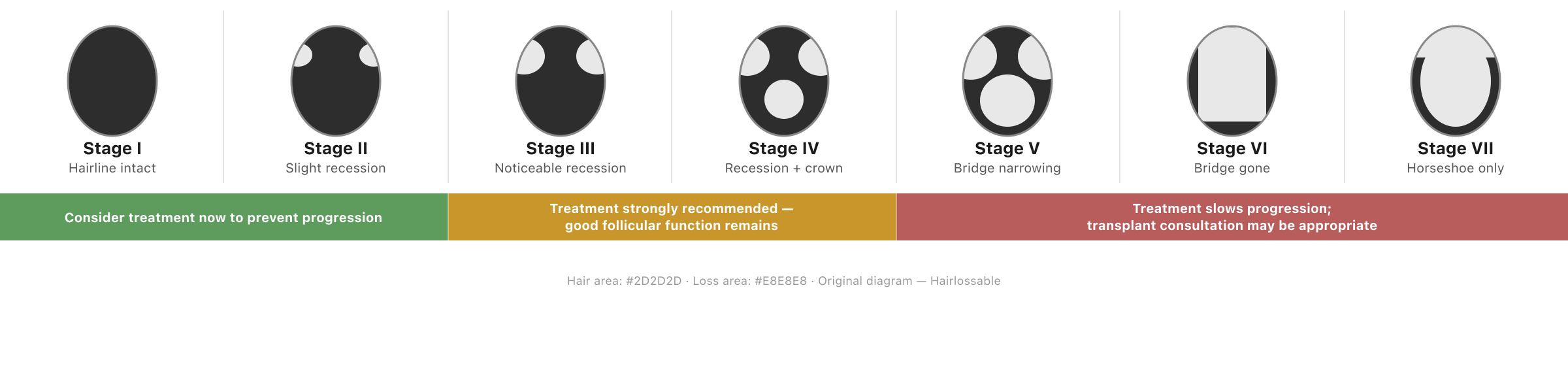
The Norwood scale classifies the progression of male pattern hair loss. Stages I–II show minimal or early recession; Stages III–IV indicate moderate progression with good remaining follicular function; Stages V–VII reflect advanced loss where medical treatment may still help preserve remaining hair but restoration planning often becomes more relevant.
Hair Loss in Women in Their 20s
Female pattern hair loss (FPHL) is less commonly diagnosed in the 20s than in men, but it is not rare — particularly in women with PCOS, insulin resistance, elevated androgens, or a strong family history of female hair loss. It can also feel more isolating: there is far less cultural space for young women to discuss hair loss openly, and most of the resources that exist are written with men in mind.
The pattern is different. FPHL in women follows the Ludwig pattern: diffuse central thinning along the part and crown, with the frontal hairline generally maintained. This is distinct from the Norwood pattern seen in men. A widening part or visibly reduced density at the top of the scalp, without a receding frontal line, is a classic early presentation.
But other causes are more common in young women. Before assuming FPHL, the following causes are particularly worth ruling out in women in their 20s:
- Telogen effluvium from contraceptive pill changes, pregnancy-related hormonal shifts, or post-illness shedding
- Iron deficiency — extremely common in young women, particularly with heavy periods; often under-diagnosed as a hair loss cause
- Thyroid dysfunction (hypo- or hyperthyroidism) — produces diffuse shedding
- PCOS-related hormonal imbalance — elevated androgens can cause both diffuse shedding and pattern loss; associated symptoms include irregular periods, acne, and hirsutism
- Traction alopecia from tight hairstyles
Blood work is essential before treating hair loss in young women: full blood count, ferritin, thyroid function (TSH, free T4), and androgens (total testosterone, DHEA-S, free androgen index) at a minimum. A GP or gynecologist can assess for PCOS if indicated.
Treatment for confirmed FPHL:
- Topical minoxidil 5% is the first-line treatment for FPHL; a 2% formulation is also used, though 5% is generally more effective
- Oral minoxidil (low-dose, off-label) is increasingly prescribed for women who find topical application difficult or experience scalp irritation
- Spironolactone (off-label anti-androgen) is used as a second-line option where a hormonal driver is identified; requires prescription and monitoring
- Finasteride is generally not used in women of childbearing age due to teratogenicity risk; it may be considered post-menopause under specialist guidance
Frequently Asked Questions
Is hair loss in your 20s normal?
Losing 50–100 hairs per day is normal — that is healthy hair cycling. Progressive thinning in a patterned distribution (temples, crown for men; central parting for women) is not “normal” in the sense of being inevitable or benign. It is AGA, which is genetic in origin but is also treatable. Approximately 25% of men begin showing AGA signs before age 21.
Will I go completely bald if I’m losing hair at 21?
Not necessarily, and not on a fixed timeline. AGA progression varies enormously between individuals. Some men lose significant density in their 20s; others progress slowly over decades. Starting treatment early with finasteride ± minoxidil significantly reduces the probability of reaching advanced Norwood stages. The trajectory is not fixed.
Should I take finasteride at 20?
If you have confirmed AGA — not TE or another reversible cause — finasteride is the most evidence-backed treatment for slowing or halting male pattern hair loss. Starting early gives it the most to preserve. However: you need a GP or dermatologist assessment first to confirm the diagnosis, rule out other causes, and discuss the side-effect profile, including the possibility of sexual side effects and the contested evidence on post-finasteride syndrome. Do not start without a medical evaluation.
Does stress cause hair loss in your 20s?
Yes — but through a specific mechanism called telogen effluvium (TE). TE causes a diffuse, all-over shedding that begins 2–3 months after a stressor (illness, rapid weight loss, intense psychological stress, major surgery). It typically resolves within 6 months once the trigger is removed. If your hair loss is patterned — concentrated at the temples or crown rather than distributed all over — it is more likely AGA. TE and AGA can co-occur, which can make diagnosis more complex.
Can I reverse hair loss in my 20s?
If it is early-stage AGA, treatment can halt progression and in some cases produce meaningful regrowth. The earlier you start, the more follicular function remains to be preserved and potentially stimulated. Late-stage AGA with extensively miniaturized or fibrosed follicles responds poorly to medical treatment alone. “Reverse” is a strong word — treatment is best understood as preservation + possible partial regrowth, not a return to your teenage hairline. For men at Norwood V–VII where medical treatment has limited scope, see our hair transplant guide.
Is minoxidil safe to use at 20?
Yes. Topical minoxidil has no specific age-based contraindication in young adults beyond its general safety profile. Common side effects include initial increased shedding (temporary, typically 4–8 weeks) and scalp irritation. Oral minoxidil carries more cardiovascular considerations and should be prescribed by a clinician. Topical minoxidil does not require a prescription in most markets.
The Bottom Line
Hair loss in your 20s is more common than you probably realized before noticing it yourself. The most common cause — androgenetic alopecia — is genetic, progressive, and won’t stop on its own. But it is also the most treatable early, with a strong evidence base behind both finasteride and minoxidil.
If you’ve been putting off dealing with this, the evidence strongly suggests that waiting works against you. Every month of untreated AGA progression is follicular function that finasteride or minoxidil cannot get back. The tools exist, the evidence is mature, and acting early is the single most effective thing you can do.
Your next steps:
- See a GP or dermatologist. Ask for a clinical assessment and blood work (ferritin, thyroid, full blood count) to rule out reversible causes.
- If AGA is confirmed, discuss finasteride ± minoxidil with your clinician. Understand the side effects before starting.
- Do not rely on supplements or shampoos to treat AGA — they do not address the DHT mechanism and the evidence for them in true AGA is weak.
- If budget or access is a barrier, topical minoxidil is OTC, affordable, and an evidence-based start while you arrange a clinical assessment.
Further Reading
- What is normal hair loss?
- Receding hairline: what it means and what to do
- Finasteride for hair loss: the complete guide
- Oral minoxidil for hair loss
- Finasteride + minoxidil combination therapy
- Telogen effluvium: diffuse hair shedding explained
- Iron deficiency and hair loss
- Hair transplant: complete guide
Medically reviewed by Dr. Ana Reyes, DO. Last updated April 2026.
This article is for informational purposes and does not constitute medical advice. If you are experiencing hair loss, please consult a GP or dermatologist for a personalized assessment.