
Melatonin is best known as a sleep hormone. But topical melatonin — applied directly to the scalp — has a growing clinical evidence base for hair loss that most people don’t know about. In a 2025 network meta-analysis ranking over-the-counter hair loss treatments, topical melatonin ranked second behind 5% minoxidil among OTC options at 24 weeks.1 This article explains what the evidence actually says, how topical melatonin works, who it might help, and how it compares to better-established treatments.
What Is Topical Melatonin and How Does It Work for Hair?
Melatonin is a hormone produced primarily by the pineal gland in response to darkness. What most people don’t know is that melatonin is also produced locally in the skin and hair follicles — and that hair follicles express melatonin receptors.
The proposed mechanisms for hair growth are distinct from melatonin’s role in sleep:
- Antioxidant protection: Melatonin is a potent antioxidant. Oxidative stress plays a role in follicle miniaturisation in androgenetic alopecia (AGA); melatonin may blunt that damage at the follicle level.
- Anagen phase extension: Research suggests melatonin may prolong the anagen (active growth) phase of the hair cycle and delay the transition to catagen (regression).
- Hormonal pathway modulation: Melatonin interacts with pathways relevant to DHT sensitivity, potentially reducing the androgenic signalling that drives AGA, though the exact mechanism is not fully established.
Topical versus oral melatonin — a critical distinction. The clinical evidence for hair loss is entirely for topical melatonin — a scalp solution or serum applied directly to the skin. Oral melatonin sleep supplements do not produce the same localised scalp concentrations studied in clinical trials. If you are considering melatonin for hair loss, you need the topical form.
What Does the Clinical Evidence Show?
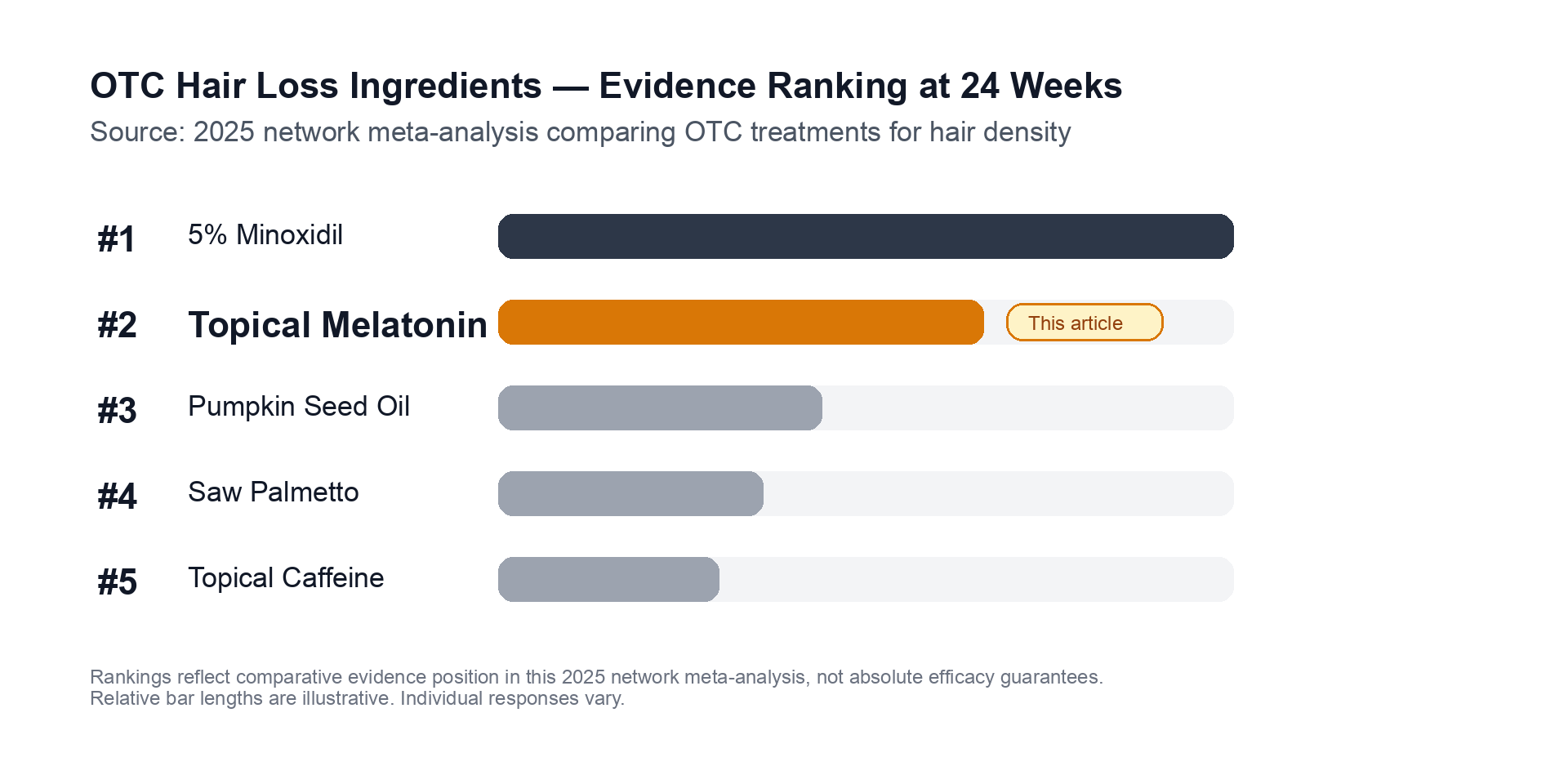
Among over-the-counter hair loss options, topical melatonin ranked second in a 2025 network meta-analysis measuring hair density outcomes at 24 weeks — behind 5% minoxidil, but ahead of most supplement-derived ingredients. Rankings reflect comparative evidence position in this analysis; individual responses vary.
The clinical picture for topical melatonin is more positive than for most supplement-derived hair ingredients — but the evidence has meaningful limitations.
The headline result: 2025 network meta-analysis
A 2025 network meta-analysis by Gupta AK et al. comparing OTC hair loss treatments on hair density outcomes at 24 weeks ranked topical melatonin second among non-prescription options, behind 5% minoxidil.1 This is the strongest comparative positioning topical melatonin has achieved in the literature.
Fischer 2012: two key datasets from one landmark paper
The most cited primary source for topical melatonin’s efficacy is Fischer TW, Trüeb RM, Hänggi G, Innocenti M, Elsner P., “Topical melatonin for treatment of androgenetic alopecia,” International Journal of Trichology, 2012 (PMCID: PMC3681103).2 This single paper reports two datasets:
Multi-centre observational study (1,800+ participants): Conducted across approximately 200 centres, this study found the negative hair-pull test rate — a measure of whether hair is in stable rather than active-shedding phase — improved from 12.2% at baseline to 61.5% at three months. That is a meaningful shift in the proportion of participants whose hair was no longer actively shedding.
35-patient AGA TrichoScan study: A smaller, controlled arm assessed hair density via TrichoScan at three and six months. Between 54.8% and 58.1% of patients showed measurable increases in hair density, with improvements ranging from 29% to 41% depending on assessment time point.
Safety data
Across the published studies, safety signals for topical melatonin are consistently mild. Occasional local scalp irritation is the most common adverse event. Systemic absorption at study concentrations is minimal — serum melatonin levels after topical application do not reach levels associated with sleep effects, and no serious adverse events have been reported.
Limitations — be realistic
- Scale: The 35-patient TrichoScan arm is underpowered by Phase III drug-trial standards
- Variable formulations: Different studies use different concentrations (0.0033%–0.1%) and vehicles, complicating comparison
- No large Phase III RCTs: The robust randomised controlled trial evidence base behind minoxidil does not exist for topical melatonin
- Condition scope: Most evidence is for AGA; less data for telogen effluvium or alopecia areata
Hairlossable Verdict
Topical melatonin has more legitimate clinical evidence than the vast majority of supplement ingredients marketed for hair loss. It is not snake oil. The 2025 network meta-analysis result — second among OTC options — is meaningful.
But it falls clearly below 5% minoxidil in direct comparisons, and the evidence base lacks the scale and rigour of established first-line treatments.
Our read: Topical melatonin is a reasonable adjunct for people who want to add something to their routine beyond minoxidil, particularly those who experience scalp irritation from minoxidil. It is not a replacement for proven first-line treatments.
| Dimension | Rating | Notes |
|---|---|---|
| Evidence quality | ★★★☆☆ | Positive signals; limited by small controlled studies and no Phase III RCTs |
| Efficacy vs minoxidil | ★★☆☆☆ | Consistently ranked below 5% minoxidil in comparative data |
| Safety profile | ★★★★★ | Very low risk; minimal systemic absorption; topical; OTC |
| Value as adjunct | ★★★☆☆ | Reasonable add-on to a core regimen; not a solo treatment |
How to Use Topical Melatonin
Topical melatonin is available as scalp solutions, sprays, and serums, mainly from European specialist brands; US availability is limited but growing.
- Apply to the scalp at night — this aligns with melatonin’s circadian biology and matches study protocols
- Typical concentrations: 0.0033%–0.1%; leave in rather than rinse out
- Commit to at least three months before evaluating response — hair growth is slow and weeks of use will not produce visible results
Who Is Topical Melatonin Best For?
Good candidates:
- People with AGA already using minoxidil who want an evidence-backed adjunct
- People who find minoxidil irritating and want a gentler companion treatment
- People who want to make data-informed ingredient choices rather than reaching for poorly evidenced supplements
Not the right choice if:
- You are looking for a sole first-line AGA treatment — evidence does not support replacing minoxidil
- You have not yet tried established first-line options — start with minoxidil first
How Does It Compare to Other Ingredients?
| Ingredient | Evidence vs topical melatonin |
|---|---|
| 5% Minoxidil | Stronger — first-line OTC; Phase III evidence; decades of data |
| Topical melatonin | #2 OTC per 2025 network meta-analysis |
| Saw palmetto | Weaker — mixed evidence; primarily DHT antagonism |
| Pumpkin seed oil | Moderate — some RCT data; fewer studies than melatonin overall |
| Caffeine shampoo | Comparable — some RCT evidence; different mechanism |
Frequently Asked Questions
Is topical melatonin the same as melatonin sleep gummies?
No. Oral sleep supplements affect systemic melatonin levels for circadian regulation. Topical melatonin is a scalp solution that acts locally on hair follicles. The two are not interchangeable.
Where can I buy topical melatonin?
It is most widely available from specialist hair care brands in European markets; US availability is growing through specialist retailers. Look for products listing melatonin at 0.003%–0.1% intended for scalp application. We do not recommend specific brands.
Does topical melatonin work for women?
The Fischer 2012 studies include both men and women. AGA (including female-pattern hair loss) is the primary studied condition.
Can I use topical melatonin with minoxidil?
Generally yes. No known pharmacokinetic interaction exists — they work via different mechanisms. Applying them at different times of day (minoxidil morning, melatonin night) minimises any product mixing.
Is it safe?
Yes, based on current evidence. Mild scalp irritation is the most common side effect. Systemic absorption at typical concentrations is minimal, so sleep disruption is not a documented concern from topical application.
Conclusion
Topical melatonin is one of the more evidence-backed ingredients in the OTC hair loss space — ranked second behind minoxidil in a 2025 OTC network meta-analysis, with supporting data from Fischer et al.’s 2012 multi-centre and TrichoScan studies. The evidence has real limitations (small controlled studies, no Phase III RCTs), but it compares favourably to most supplement-class hair ingredients.
For those looking to supplement their core regimen with something that has genuine clinical data, topical melatonin is a defensible choice. Use it consistently for at least three months to evaluate effect. If you have significant AGA, see a dermatologist — evidence-based treatment (minoxidil, and where appropriate, finasteride or oral minoxidil) should be the foundation of your regimen.
References
Footnotes
-
Gupta AK, Bamimore MA, Talukder M. “Network meta-analysis of over-the-counter treatments for androgenetic alopecia.” J Cosmet Dermatol. 2025 Oct;24(10):e70483. DOI: 10.1111/jocd.70483. PMID: 41051009. PMCID: PMC12498493. ↩ ↩2
-
Fischer TW, Trüeb RM, Hänggi G, Innocenti M, Elsner P. “Topical melatonin for treatment of androgenetic alopecia.” Int J Trichology. 2012 Oct;4(4):236-45. DOI: 10.4103/0974-7753.111199. PMID: 23766606. PMCID: PMC3681103. ↩