Male pattern baldness is the most common cause of hair loss in men. If you have noticed your hairline receding, your crown thinning, or both, there is a very good chance you are dealing with androgenetic alopecia (AGA) — the medical term for this condition. It affects a significant proportion of men across their lifetimes, it has well-understood causes, and there are treatments with meaningful clinical evidence behind them.
This guide explains what male pattern baldness is, why it happens, how to recognise the different stages, what treatments genuinely work, what to skip, and when it is worth seeing a doctor. Because Hairlossable covers every relevant treatment in detail, you will find links throughout to the deeper evidence breakdowns.
What Is Male Pattern Baldness?
Androgenetic alopecia is a genetically driven, hormone-mediated progressive miniaturisation of hair follicles in androgen-sensitive scalp regions. In plain English: certain hair follicles are genetically programmed to respond to androgens (male sex hormones) in a way that makes them shrink over time, producing progressively thinner, shorter, and eventually barely visible hairs before they stop producing hair entirely.
The “male pattern” part refers to the characteristic distribution — temples, crown, and midscalp — while the sides and back of the scalp (the occipital and parietal regions) are typically androgen-resistant and retain hair even with advanced loss. This is the region from which donor hair is taken in hair transplant surgery.
How Common Is It?
Very common. Estimates vary across studies, but the general picture is well established: male pattern baldness affects a substantial proportion of men, with prevalence rising steeply with age. Roughly half of men show some degree of AGA by their fifties, and the majority will show it by their seventies and eighties. It can also begin in the twenties — early-onset hair loss is not rare, and for men who start losing hair in their twenties, progression tends to be more significant over time if untreated.
AGA occurs across all ethnicities, though prevalence varies — higher rates are consistently reported in men of European ancestry compared to men of East Asian or African ancestry, likely reflecting genetic differences in androgen receptor sensitivity.
Why Does It Happen? The DHT Mechanism
The driver of male pattern baldness is dihydrotestosterone (DHT) — a more potent androgen derived from testosterone via an enzyme called 5-alpha reductase.
Here is the basic sequence:
- Testosterone is converted to DHT by 5-alpha reductase (primarily type II in hair follicles, type I in sebaceous glands).
- DHT binds to androgen receptors in susceptible hair follicles.
- Over repeated cycles of hair growth (each cycle taking months to years), the follicle miniaturises — the growth (anagen) phase shortens, the resting (telogen) phase lengthens, and each hair produced is thinner and lighter.
- Eventually, the follicle produces only vellus (fine, nearly invisible) hairs, or stops producing hair altogether.
The key word is susceptible. Not all follicles respond this way. The follicles on the top of the scalp carry more androgen receptors and are genetically predisposed to this miniaturisation response. The follicles on the sides and back generally are not.
Genetics determines which follicles are susceptible. AGA is polygenic — many genes contribute — and inheritance can come from either side of the family, not just the maternal grandfather as the old myth suggests. Our full explainer on DHT and hair loss covers the mechanism in more detail, including why some men with high testosterone do not go bald and others with average testosterone do.
The Norwood Scale: What Stage Are You?
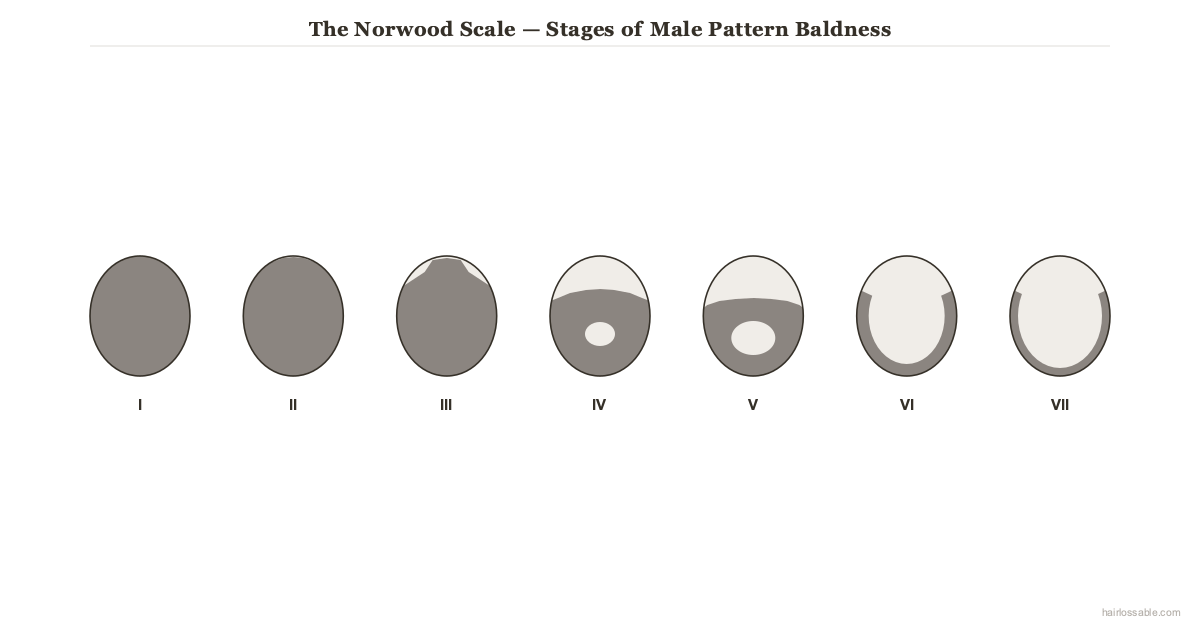 The Norwood-Hamilton scale maps male pattern baldness from Stage I (full hairline) through Stage VII (only a horseshoe fringe remains). Most men who seek treatment are Stage II–IV — the earlier treatment starts, the more there is to preserve.
The Norwood-Hamilton scale maps male pattern baldness from Stage I (full hairline) through Stage VII (only a horseshoe fringe remains). Most men who seek treatment are Stage II–IV — the earlier treatment starts, the more there is to preserve.
The Hamilton-Norwood scale is the standard classification system for male pattern baldness. It runs from Type I to Type VII:
- Type I — Minimal or no recession. A young adult hairline.
- Type II — Slight recession at the temples. Early-stage AGA.
- Type III — Deeper temple recession that forms an M-shape. The earliest stage many men first notice and seek help.
- Type III Vertex — Recession similar to Type III but with additional thinning at the crown.
- Type IV — More significant temple recession plus obvious crown thinning; the two areas remain separated by a band of hair.
- Type V — The temple and crown thinning areas begin to merge.
- Type VI — The two areas have merged; only a horseshoe band of hair remains on the sides and back.
- Type VII — The most advanced stage; the remaining horseshoe band is narrow and sits low on the scalp.
Knowing your approximate Norwood stage matters for treatment decisions. Men at earlier stages (II–IV) generally respond better to medical treatments. Men at stages V–VII have fewer viable follicles remaining on the scalp, which limits how much medical therapy can achieve — though hair transplant surgery becomes more relevant at these stages.
Is Male Pattern Baldness Reversible?
This is worth addressing directly. Male pattern baldness cannot be “cured” — there is no treatment that permanently resets follicle genetics or removes the underlying susceptibility to DHT. What treatments can do is:
- Slow or stop progression (the main goal of early intervention)
- Partially reverse miniaturisation in follicles that have shrunk but not yet become fully dormant
- Restore cosmetically significant density in some men, particularly with early treatment
The earlier you start treatment, the more you have to protect. Hair that has been completely lost for many years is much harder (and often impossible) to recover with medical therapy alone. This is why early intervention consistently produces better outcomes than waiting until loss is advanced.
Treatment is also ongoing. Stopping medication typically means the benefits reverse over the following months to years.
First-Line Treatments: What the Evidence Says
These are the treatments with the strongest clinical evidence for male AGA.
Minoxidil (Topical)
Minoxidil is the only topical treatment approved by the FDA for male pattern baldness. It was originally developed as an oral antihypertensive; scalp application was adopted after patients using it orally noticed increased hair growth.
How it works in the follicle is not fully established, but the leading explanation involves minoxidil acting as a potassium channel opener, increasing blood flow to the follicle and likely prolonging the anagen (growth) phase. It may also have direct effects on follicular keratinocytes.
Clinical trials show topical minoxidil (2% or 5%) produces measurable increases in hair count and density in a meaningful proportion of men with AGA, with the 5% formulation showing superior efficacy to 2%. Response is variable — not everyone responds equally well, and about 10–15% of users see little benefit.
Key practical notes:
- It typically takes four to six months of consistent use to see meaningful results.
- Initial shedding is common in the first one to two months — this is a normal sign of follicle cycling, not treatment failure. It typically resolves within eight weeks as follicle cycling settles.
- Application must be maintained indefinitely. Stopping reverses any gains within months.
Oral Minoxidil
Low-dose oral minoxidil (typically 2.5–5mg daily for men, lower for women) has gained significant clinical traction in recent years as an alternative to topical application for men who find topical formulations inconvenient or have inadequate response.
Evidence from dermatology trials and case series supports its efficacy for AGA, and some data suggest it may outperform topical minoxidil in terms of hair density outcomes, though direct head-to-head RCT comparisons are limited. Our full guide to oral minoxidil covers the evidence, how it differs from topical formulations, and the side effect profile — which includes hypertrichosis (unwanted body hair growth) and, at higher doses, cardiovascular effects.
Oral minoxidil is prescription-only in most countries. Discuss with your doctor whether it is appropriate for you.
Finasteride
Finasteride (1mg daily, oral) is the other FDA-approved treatment for male AGA. It works by inhibiting type II 5-alpha reductase, the enzyme primarily responsible for DHT production in scalp follicles. In clinical trials, finasteride reduces scalp DHT levels by approximately 60–70%.
The Phase III RCTs supporting finasteride’s approval showed statistically significant increases in hair count versus placebo over two and five years, with the majority of men experiencing stabilisation or improvement. Some men see modest regrowth, particularly at earlier stages.
Our detailed finasteride guide covers the clinical evidence, how to use it, and what to expect. Finasteride’s side effect profile — including the sexual side effects (reduced libido, erectile dysfunction, ejaculatory changes) that affect a minority of users — is covered in full in its own article. These side effects are real, and anyone considering finasteride should read that information before starting. Like minoxidil, finasteride requires ongoing use; stopping it reverses most of its benefit within twelve months.
Topical Finasteride
For men who want the DHT-reducing mechanism of finasteride with reduced systemic exposure, topical finasteride formulations are available and increasingly prescribed. Studies show topical application can achieve meaningful reductions in scalp DHT with lower serum finasteride concentrations compared to oral dosing. Our guide to topical finasteride explains the evidence and how it compares to the oral form.
Dutasteride
Dutasteride inhibits both type I and type II 5-alpha reductase, reducing DHT more completely than finasteride (by 90%+ versus ~70% for finasteride). It is approved for AGA in some countries (Japan, South Korea) and prescribed off-label in others.
A 2025 network meta-analysis (Journal of Cosmetic Dermatology, Gupta et al.) ranked dutasteride above finasteride and minoxidil monotherapy for hair density outcomes. However, the greater DHT suppression comes with a longer half-life and potentially more persistent side effects if they occur.
Our dutasteride guide covers the evidence and the key clinical considerations. This is a prescription medication; a discussion with your doctor is essential before starting.
Combination Therapy: Minoxidil + Finasteride
For many men, combining minoxidil and finasteride offers better outcomes than either alone, since the two treatments work through entirely different mechanisms — minoxidil acting primarily on follicle growth cycles and blood flow, finasteride reducing the androgenic stimulus driving miniaturisation. Several studies support superior efficacy for the combination.
Our combination therapy guide covers what the evidence says about combination regimens, including fixed-dose combination topical products.
Second-Line and Adjunct Treatments
These options have emerging or supporting evidence but are generally considered adjuncts rather than primary therapies. None are substitutes for the first-line options above.
Low-Level Laser Therapy (LLLT)
Laser devices (combs, caps, headbands) using specific wavelengths of red or near-infrared light have received FDA clearance for hair loss treatment, with several controlled trials showing modest improvements in hair density with consistent use. The mechanism likely involves photobiomodulation — cellular energy effects on follicular metabolism.
Results vary and are generally more modest than finasteride or minoxidil, but LLLT has a mild side effect profile and may complement first-line treatment.
Platelet-Rich Plasma (PRP)
PRP involves drawing a small amount of the patient’s own blood, concentrating the platelet-rich fraction, and injecting it into the scalp. Platelets contain growth factors (including PDGF and VEGF) that may stimulate follicular activity.
Controlled trials show encouraging results for AGA, though study quality varies and there is no standardised protocol — PRP formulations and injection protocols differ significantly between studies and clinics, making outcomes hard to compare directly. It is typically used as an adjunct to medical therapy rather than a standalone treatment. Full PRP guide here.
Microneedling and Dermarolling
Microneedling (using a dermaroller or dermapen) creates micro-injuries in the scalp that may stimulate wound-healing growth factors and potentially enhance absorption of topical treatments like minoxidil. Several RCTs have shown that microneedling plus minoxidil outperforms minoxidil alone.
Our microneedling guide and dermarolling guide cover the evidence for at-home and in-clinic protocols.
Ketoconazole Shampoo
Ketoconazole is an antifungal with weak anti-androgenic properties. Used as a shampoo (1–2%), small studies suggest it may have a mild hair-density benefit in AGA, possibly through local androgen receptor interference. It is often used as an adjunct — cheap, low-risk, and potentially complementary — rather than as a primary treatment.
Scalp Massage
Consistent scalp massage may have a modest benefit via mechanical stretching of follicular cells, as suggested by a small Japanese study. It is unlikely to produce clinically significant results on its own but costs nothing and has no downside.
Surgical Options: Hair Transplant
Hair transplant surgery is the most definitive intervention for male pattern baldness and the only option that addresses areas where follicles have already been lost. It does not stop ongoing hair loss — medical therapy should continue post-transplant to protect non-transplanted hair.
Modern transplant surgery uses two main techniques:
- FUE (Follicular Unit Extraction) — individual follicular units are extracted from the donor area and implanted in recipient sites. Minimal linear scarring; faster recovery.
- FUT (Follicular Unit Transplantation / strip method) — a strip of scalp is removed from the donor area, follicular units are dissected under a microscope, and implanted. More grafts per session; leaves a linear scar.
Both techniques use donor follicles from the androgen-resistant sides and back of the scalp. Because these follicles retain their genetic resistance after transplant, results are generally permanent — though the surrounding non-transplanted hair continues to be susceptible to AGA.
Candidacy depends on donor supply, degree of loss, and realistic expectations about coverage. Our complete hair transplant guide covers candidacy, technique comparison, what to expect, and how to evaluate a surgeon.
What Does Not Work (or Barely Does)
Being honest about what lacks convincing evidence is as important as covering what works.
Biotin
Biotin supplementation is widely marketed for hair growth but has essentially no evidence of benefit in people who are not biotin-deficient — and biotin deficiency is rare. If you eat a reasonably varied diet, you almost certainly do not need biotin supplements for your hair. Full evidence review here.
Saw Palmetto
Saw palmetto is often marketed as a “natural DHT blocker.” It has some anti-androgenic activity, but clinical evidence for meaningful AGA benefit is weak and inconsistent. It is not a reliable alternative to finasteride or dutasteride. Evidence review.
Pumpkin Seed Oil
Some trial data (a small, single-blind RCT) showed a benefit for pumpkin seed oil supplementation in male AGA, but the study has methodological limitations and has not been independently replicated. It is not a substitute for established treatments. Evidence review.
Rosemary Oil
One small trial found rosemary oil comparable to 2% minoxidil — but this comparison has been widely overclaimed relative to the study’s limitations (small sample, single trial, different application frequency). Rosemary oil may have mild benefit; it is not an equivalent alternative to 5% minoxidil or finasteride.
Caffeine Shampoos
Caffeine has demonstrated some in vitro effects on follicular cells, but whether this translates to meaningful clinical hair regrowth from a rinse-off shampoo remains unconvincing.
Hair Vitamins and Supplements
Most commercial “hair growth supplements” are not supported by clinical evidence for AGA and target a common anxiety about deficiency. If you have a confirmed nutritional deficiency (iron, vitamin D, zinc, B12, protein), correcting it matters — but supplementing randomly when you are not deficient is unlikely to regrow hair. For a broad review of supplements marketed for hair loss, see our supplements guide.
Common Myths About Male Pattern Baldness
”Wearing hats causes baldness”
Hats do not cause or worsen male pattern baldness. Genetics and DHT determine follicle fate, not headwear. A hat tight enough to cause traction on the scalp consistently over years could theoretically contribute to a different type of hair loss (traction alopecia), but normal hat-wearing is not a factor in AGA.
”Masturbation causes hair loss”
Persistent in online forums, this claim has no clinical evidence to support it. The mechanism proposed — that ejaculation raises testosterone, which is converted to DHT — does not hold up: the transient hormonal changes involved are minor and would not drive follicular miniaturisation.
”Hair loss comes from your mother’s side”
The androgen receptor gene is X-linked, so early genetics research suggested the maternal line mattered more. But AGA is polygenic — many genes on many chromosomes contribute. Baldness can and does come from either side of the family, and the mother’s-father rule is too simplistic to be a reliable predictor.
”High testosterone causes baldness”
DHT sensitivity — not testosterone levels per se — drives AGA. Some men with below-average testosterone go bald; some men with high testosterone do not. Serum testosterone level is not a useful predictor of AGA risk. The relevant factors are androgen receptor sensitivity and 5-alpha reductase activity in scalp follicles, both of which are genetically determined.
”Creatine causes hair loss”
A single small study in rugby players found that creatine supplementation raised DHT relative to testosterone. This has been extrapolated into a widespread concern. The study has not been replicated in subsequent trials, and there is currently no clinical evidence that creatine at normal supplementation doses causes or accelerates male pattern baldness.
”Stress causes male pattern baldness”
Significant physical or emotional stress can cause a diffuse, temporary shedding called telogen effluvium, which is a different condition from AGA. Telogen effluvium typically resolves once the stressor is removed. It can, however, occur concurrently with AGA and is sometimes mistaken for it.
When to See a Doctor
You do not need a symptom threshold to see a doctor about hair loss — any time you are bothered by it is a reasonable time to get an assessment. That said, certain patterns particularly warrant professional evaluation:
- Rapid or sudden onset — AGA typically progresses gradually over years; rapid loss warrants investigation for other causes including autoimmune conditions or nutritional deficiencies.
- Diffuse thinning across the whole scalp (rather than the characteristic AGA pattern) — this suggests telogen effluvium, thyroid dysfunction, iron deficiency, or other systemic causes.
- Patchy loss — patchy hair loss, especially in well-demarcated round or oval patches, may be alopecia areata, which has a different cause and treatment pathway.
- Scalp symptoms — significant itching, scaling, pain, or tenderness alongside hair loss may indicate seborrheic dermatitis, scalp psoriasis, or scarring alopecia, which require different management.
- Before starting any treatment — finasteride, dutasteride, and oral minoxidil are prescription medications in most countries and should be started with professional oversight, not self-prescribed without guidance.
Our guide on when to see a doctor about hair loss covers the full triage in more detail.
Frequently Asked Questions
Will my hair grow back if I start treatment? Possibly, but regrowth is not guaranteed. The more realistic expectation for most men — especially those with established loss — is stabilisation rather than significant regrowth. Earlier treatment is associated with better outcomes. Maintaining hair you have is usually more achievable than recovering hair that has been lost for years.
Which treatment should I start with? That depends on your health, risk tolerance, and severity of loss. Topical minoxidil is available over the counter and is the lowest-barrier starting point. Finasteride requires a prescription but has strong evidence for slowing progression. Combining the two produces better results than either alone for most men. Speak to your GP or a dermatologist about what fits your situation — treatment decisions for prescription medications should involve a clinician.
How long do I need to stay on treatment? Indefinitely, if you want to maintain the benefits. Stopping treatment typically leads to progression resuming. Most men who start effective treatment in their twenties or thirties treat it as a long-term management strategy, the same way one would manage any chronic but benign condition.
Is a hair transplant permanent? Transplanted follicles are resistant to DHT and generally provide permanent results. However, non-transplanted native hair continues to be susceptible to AGA and will likely continue to thin without medical therapy. Most surgeons recommend continuing medical treatment after a transplant to protect surrounding hair.
Can male pattern baldness be prevented? Not entirely — genetics determines susceptibility. But starting medical treatment early (at signs of recession or thinning) can significantly slow progression and prevent much of the cosmetically significant loss from ever occurring.
The Bottom Line
Male pattern baldness is common, progressive, and driven by a well-understood combination of genetics and DHT. It is not reversible, but it is very much manageable — particularly when treated early.
The treatments with the strongest evidence are:
- Minoxidil (topical or oral) — stimulates follicular activity; works best as long-term maintenance
- Finasteride — reduces DHT at the follicle level; strong evidence for slowing progression
- Dutasteride — more complete DHT suppression than finasteride; used in some countries for AGA
- Combination therapy — the most effective medical approach for most men
- Hair transplant — the definitive surgical option for areas with established loss
Everything else sits in a spectrum from “modest adjunct” to “no meaningful evidence.” Being clear-eyed about that spectrum matters, because the supplement and cosmetic industry invests heavily in marketing products with weak or no evidence to people who are anxious about their hair.
If you are noticing hair loss and want to do something about it, the most useful first step is understanding what you are dealing with — and then having a conversation with a doctor about which evidence-based options fit your situation.
This article is intended as an educational overview. It does not constitute medical advice. Speak with a qualified healthcare professional before starting any treatment for hair loss, including prescription medications such as finasteride, dutasteride, and oral minoxidil.
Related Reading
- DHT and hair loss: the full mechanism explained
- Finasteride for hair loss: evidence, dosing, and what to expect
- Finasteride side effects: the complete picture
- Topical finasteride: lower systemic exposure, same mechanism
- Oral minoxidil: evidence, dosing, and side effects
- Minoxidil shedding: what is normal and what is not
- Dutasteride for hair loss
- Minoxidil and finasteride together: what the evidence says
- Hair transplant: the complete guide
- PRP for hair loss
- Microneedling for hair loss
- Dermarolling for hair loss
- Hair loss in your 20s: what is normal and what to do
- When to see a doctor about hair loss
- Do hair vitamins work?
- Hair loss supplements: the evidence
- Saw palmetto for hair loss
- Pumpkin seed oil for hair loss
- Rosemary oil for hair loss
- Biotin for hair growth: the evidence
- Creatine and hair loss
- Wearing hats and hair loss
- Masturbation and hair loss
- Stress and hair loss
- Scalp massage for hair growth
- Caffeine shampoo and hair loss