
Minoxidil for Women: A Complete Treatment Guide
Minoxidil is the most widely used treatment for female pattern hair loss. It is FDA-approved, has decades of clinical evidence behind it, and is available in formulations designed specifically for women. It also comes with real limitations and real risks — particularly if you are pregnant or thinking about becoming pregnant.
This guide covers all three minoxidil options available to women: 2% topical solution, 5% topical foam, and low-dose oral minoxidil. It explains what the evidence says about each, what side effects to expect, and how to have a more informed conversation with your doctor or dermatologist.
Does minoxidil work for women?
Yes — for the right condition, with the right expectations.
Topical minoxidil is FDA-approved for female pattern hair loss (FPHL), the most common cause of hair thinning in women. Multiple clinical trials confirm it slows progression and, for many women, promotes some regrowth of miniaturised hairs.
The most commonly cited figure from the pivotal FDA approval trials: up to around 60% of women saw noticeably thicker hair after eight months of consistent use of 2% solution twice daily, compared with placebo. Studies measuring actual hair counts confirm that improvement occurs in the majority of treated women.
What minoxidil does not do is cure FPHL. It does not change the underlying genetic susceptibility or hormonal mechanism that drives the condition. It works while you take it — and hair loss typically resumes within three to six months of stopping.
If you have a different type of hair loss — such as alopecia areata, telogen effluvium from a nutritional deficiency, or hair loss caused by a thyroid condition — minoxidil may not be the right treatment, or may need to be combined with treating the underlying cause. A diagnosis from a dermatologist or GP is important before starting any treatment.
What minoxidil options are available for women
There are three formulations relevant to women, and they differ meaningfully in how they are taken, their regulatory status, and their side-effect profile.
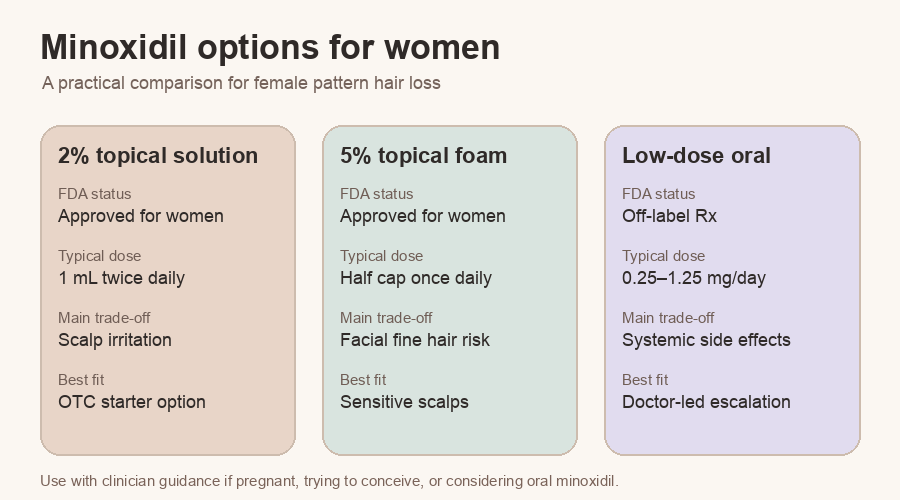
2% topical minoxidil solution (FDA-approved for women, twice daily)
This is the original formulation studied in the pivotal FDA approval trials for women with FPHL. It is applied to the scalp twice daily and is available over the counter in many markets.
The solution formulation typically contains propylene glycol as a carrier ingredient. A minority of users experience contact dermatitis — scalp irritation or redness — as a reaction to propylene glycol rather than to minoxidil itself. If this happens, switching to the foam formulation (which is usually propylene glycol-free) often resolves it.
5% topical minoxidil foam (FDA-approved for women, once daily)
5% minoxidil foam received FDA approval for women at a once-daily dose. It was originally developed for men but has been approved for women at this different dosing schedule.
Some evidence suggests the 5% concentration may perform better than 2% for some women, though direct head-to-head trial data in women specifically is more limited than for men. The foam formulation avoids the propylene glycol issue and is generally better tolerated for scalp-sensitive users.
The trade-off: the 5% formulation carries a slightly higher rate of facial hypertrichosis (fine hair growth on the forehead, cheeks, or upper lip) compared with 2%. This remains manageable for most users — see the side effects section below.
Low-dose oral minoxidil (off-label, prescription-only)
Oral minoxidil was originally developed as a blood pressure medication. It is not FDA-approved for hair loss — it is prescribed off-label for this purpose — and it requires a prescription.
At the doses used for hair loss in women (typically 0.25–1.25 mg daily, far below the antihypertensive doses of 5–40 mg), oral minoxidil has become an increasingly common option. Dermatologists have been using it off-label for several years, and the evidence has been building steadily.
January 2025: the key evidence milestone. In January 2025, an international panel of hair loss experts published a formal expert consensus in JAMA Dermatology endorsing clinical guidelines for the use of low-dose oral minoxidil for women with hair loss. This is the most significant recent development in the evidence base for oral minoxidil and represents the strongest formal endorsement the treatment has received from the dermatology community to date.
Supporting that consensus: a descriptive study of 148 women treated with low-dose oral minoxidil found that 79.7% showed clinical improvement, with 15.5% showing marked improvement. A 2022 systematic review found improvement rates of 61–86% for female pattern hair loss across multiple oral minoxidil studies.
Oral minoxidil has practical advantages over topical: no application to the scalp, systemic distribution that reaches areas beyond the crown, and no adherence challenges with fine or dense hair. Its disadvantages — systemic side effects, prescription requirement, and reproductive health contraindications — are covered in the sections below.
How minoxidil works for FPHL
Minoxidil is a potassium channel opener. In the hair follicle, it prolongs the anagen (active growth) phase of the hair cycle and may promote recovery of follicles that have undergone miniaturisation — the progressive thinning of individual hair strands that characterises FPHL.
The exact molecular mechanism at the follicle level is not fully established. What is well-established is the clinical effect: minoxidil increases hair density, diameter, and growth rate in the majority of people who use it consistently for FPHL.
One important distinction: minoxidil does not work on the androgen pathway that drives FPHL in many women. Treatments like spironolactone target that pathway directly. Minoxidil works by stimulating follicle activity independently of androgens — which is why it can be used alongside anti-androgen treatments when needed, often with additive benefit.
What results to expect — and when
Initial shedding (weeks 1–8)
Many women experience increased hair shedding in the first four to eight weeks of starting minoxidil. This is known informally as the “dread shed” and is a known, temporary effect: the drug pushes resting follicles into a synchronised transition to active growth, and some hairs shed before the new growth comes in.
This is normal. It does not mean minoxidil is making things worse. Do not stop minoxidil because of initial shedding — stopping and restarting is harder on the hair cycle and delays results.
Stabilisation (months 2–4)
Most women notice that shedding slows and stabilises by months two to four. This is often the first meaningful signal that the treatment is working, even before visible density improvement is apparent.
Visible improvement (months 4–8 and beyond)
Meaningful visible improvement in hair density typically takes four to eight months. Hair grows at approximately one centimetre per month — results cannot be rushed. If you are assessing results, six months of consistent use is the minimum reasonable evaluation window, with twelve months giving a fuller picture.
Taking photographs in consistent lighting every eight to twelve weeks is a more reliable tracking method than daily inspection, which is unreliable because hair density is affected by styling, washing, lighting, and mood.
Ongoing use
This is the most important expectation to set at the start: minoxidil must be continued indefinitely. Hair loss returns, typically within three to six months of stopping, as the treatment effect wears off. Minoxidil for FPHL is maintenance treatment, not a course. If you are not prepared to use it long-term, it is worth discussing alternatives or combination approaches with your doctor.
Side effects women should know about
Topical minoxidil
Scalp irritation and contact dermatitis. Usually caused by propylene glycol in the solution formulation, not the minoxidil itself. Switch to foam if this is a problem.
Initial shedding. Described above — normal and temporary.
Facial hypertrichosis. Fine, downy hair growth on the forehead, temples, cheeks, or upper lip. This is the most commonly reported cosmetic side effect and is more likely with the 5% concentration than 2%. It occurs in a minority of users — estimates vary but roughly 5–10% with oral minoxidil at low doses, and less commonly with topical. It is usually manageable with hair removal and typically resolves if the dose is reduced or treatment is stopped.
Scalp dryness or flaking. Common and manageable with a gentle, sulphate-free shampoo.
Oral minoxidil (additional considerations)
Facial hypertrichosis. More common with oral than topical at equivalent efficacy doses. At 0.25–1.25 mg/day, it is manageable but real and must be disclosed to every patient before starting.
Fluid retention and oedema. Low-dose oral minimises this, but women with cardiac conditions, renal impairment, or hypertension need to discuss with their doctor before starting and should start at the lowest dose (0.25 mg). Ankle swelling is the most commonly reported form.
Hypotension and dizziness. Can occur, particularly at higher doses or in women who already have low blood pressure. Taking oral minoxidil in the evening may help reduce the impact of any blood pressure effect.
Pericardial effusion. Extremely rare at low doses — this is a concern at the antihypertensive doses of 5–40 mg, not at 0.25–1.25 mg. It is not typically a clinical concern at hair loss doses, but the prescribing doctor should be informed of any cardiac history.
Tachycardia. Rare at low doses. Women with a cardiac history may benefit from a baseline cardiovascular assessment before starting oral minoxidil.
Pregnancy and reproductive health — read this first if you are pregnant or planning to be
Oral minoxidil is contraindicated in pregnancy. This is the most important safety point in this article.
Oral minoxidil is teratogenic in animal studies. Human data is limited, but the risk is considered sufficient to classify oral minoxidil as contraindicated in pregnancy (equivalent to Category X under the former FDA classification system).
Women of childbearing age who are prescribed oral minoxidil:
- Should be using reliable contraception while taking oral minoxidil
- Must stop oral minoxidil immediately if they become pregnant and contact their prescribing doctor
- Should not start oral minoxidil if they are pregnant, trying to conceive, or not using reliable contraception, without an explicit discussion with their prescriber about the risks
Breastfeeding: Minoxidil passes into breast milk in small amounts. Both oral and topical minoxidil are generally not recommended during breastfeeding. Discuss with your doctor.
Topical minoxidil in pregnancy: Systemic absorption from topical application is substantially lower than oral, which reduces but does not eliminate the theoretical risk. If you are currently using topical minoxidil and become pregnant or are planning to become pregnant, stop use as a precaution and consult your doctor or midwife. The prescribing decision is theirs — but stopping while you seek guidance is the safe default.
Oral vs topical: how to decide (with your doctor)
This is not a decision you should make alone. The right choice depends on your medical history, your hair loss pattern, your lifestyle, and your reproductive plans. What follows is a guide to the conversation — not a prescription.
Topical minoxidil may be the better starting point when:
- You are pregnant, planning pregnancy, or not using reliable contraception
- You have cardiovascular, renal, or blood pressure conditions
- You prefer OTC access (2% solution is available without a prescription in many markets)
- Your hair loss is primarily in the crown/top region where topical application is practical
Oral minoxidil may be worth discussing with your doctor when:
- Topical adherence is difficult because of hair texture, density, or lifestyle
- You have diffuse shedding that extends beyond the crown
- You have experienced scalp irritation with topical formulations
- A dermatologist recommends it as a first-line option based on your specific presentation
- You have already tried topical consistently and response has been limited
In practice, many dermatologists now offer low-dose oral minoxidil as a first-line or early option for women with FPHL, particularly since the January 2025 JAMA Dermatology consensus. This does not mean it is right for everyone. The prescription requirement is not just bureaucratic — a prescriber assessment helps catch the cardiovascular and reproductive contraindications that make oral minoxidil unsuitable for some women.
Can you use both?
Some women use both topical and oral minoxidil simultaneously. The evidence on combination use is limited, and the risk of cumulative side effects — particularly hypertrichosis and cardiovascular effects — is real. This is a clinical decision, not a DIY choice.
What happens if you stop minoxidil?
Hair loss returns. Not immediately — typically within three to six months — but it does return as the treatment effect wears off. Minoxidil does not alter the underlying genetics or hormonal mechanisms driving FPHL, so the condition continues in its absence.
This is not a reason not to start. It is a reason to understand what you are signing up for before you do. For a chronic, progressive condition like FPHL, ongoing treatment to maintain ongoing benefit is clinically accepted and widely used — the same logic applies to other maintenance treatments for chronic conditions.
If you decide to stop minoxidil for any reason (pregnancy, side effects, preference), doing so gradually rather than abruptly may reduce the intensity of the rebound shed. Talk to your dermatologist before stopping, especially if you have been on oral minoxidil.
Summary: what the evidence says
| 2% topical solution | 5% topical foam | Oral (0.25–1.25 mg) | |
|---|---|---|---|
| FDA approval for women | Yes (twice daily) | Yes (once daily) | No — off-label |
| Prescription required? | Not in most markets | Not in most markets | Yes |
| Key evidence | Pivotal FDA trials; ~60% see improvement at 8 months | FDA approval; likely similar or better than 2% | 79.7% clinical improvement (Rodrigues-Barata et al., 2020); 2025 JAMA Derm expert consensus |
| Facial hypertrichosis risk | Low | Slightly higher than 2% | Most common side effect (~5–10%) |
| Safe in pregnancy? | Avoided as precaution | Avoided as precaution | Contraindicated |
| Cardiovascular caution needed? | Minimal with topical | Minimal with topical | Yes — discuss with prescriber |
Questions women commonly ask
Can women use 5% minoxidil? Yes — 5% topical foam is FDA-approved for women at once daily dosing. Many dermatologists also prescribe 5% solution off-label. The evidence suggests it may perform better than 2% for some women; the trade-off is a slightly higher rate of facial hypertrichosis.
How long does minoxidil take to work for women? Allow six months of consistent use before evaluating results. Some women see early signs of improvement (reduced shedding, early regrowth) at two to four months; meaningful visible density improvement typically takes four to eight months. Twelve months gives the most complete picture.
Can I stop minoxidil if I become pregnant? You should. If you are on oral minoxidil and become pregnant, stop immediately and contact your prescribing doctor. Oral minoxidil is contraindicated in pregnancy. Topical minoxidil should also be stopped and discussed with your doctor.
What is the best minoxidil for women with FPHL? There is no single best option — it depends on your medical history, lifestyle, and preferences. Topical 2% or 5% foam are well-evidenced OTC options. Oral minoxidil is increasingly used under prescription. A dermatologist can help determine which suits your situation.
Can I use minoxidil and spironolactone together? Yes — they work through different mechanisms and can be used together. This is a clinical decision. Discuss with your dermatologist. A dedicated Hairlossable spironolactone guide will cover anti-androgen treatment in more detail once it is published.
The bottom line
Minoxidil works for female pattern hair loss. The evidence is strong across all three formulations — topical 2%, topical 5% foam, and low-dose oral. The January 2025 JAMA Dermatology expert consensus on oral minoxidil represents a significant step forward in the formal recognition of this treatment for women.
Using minoxidil effectively means:
- Starting with a proper diagnosis — not all hair loss responds to minoxidil
- Setting realistic expectations — results take months; treatment is indefinite
- Understanding the pregnancy contraindication for oral minoxidil before starting
- Using a prescription-only route for oral minoxidil; not self-prescribing
- Being consistent — minoxidil only works while you use it
If you have been experiencing hair loss and want to understand your options, the next step is a conversation with a dermatologist or GP who can confirm the diagnosis and recommend the most appropriate treatment.
This article is for information only and does not constitute medical advice. Minoxidil treatment should be discussed with a qualified healthcare professional, particularly oral minoxidil, which requires a prescription and involves cardiovascular and reproductive health considerations.