Traction Alopecia: Can It Grow Back? Early Signs, Reversibility Timeline, and What Actually Works
This article is for informational purposes. For staging and personalised treatment decisions, consult a board-certified dermatologist.
Traction alopecia is one of the few types of hair loss that is highly likely to be reversible — if you catch it early and stop the cause. The single best treatment is also the simplest: changing your hairstyle. Unlike most forms of hair loss, you don’t need a prescription, a clinic visit, or a complex treatment regimen. You need to reduce the tension on your hairline.
This guide explains why traction alopecia happens, what the early warning signs look like, how to tell whether your case is still reversible, and what the evidence actually says about treatments beyond the hairstyle change — including the honest verdict on minoxidil.
What Is Traction Alopecia?
Traction alopecia (TA) is hair loss caused by chronic mechanical tension on hair follicles from tight hairstyles. The repeated pulling force damages follicles over time: sustained tension causes inflammation around the follicle root, progressive miniaturisation of the hair shaft, and — if the cause is not removed — eventual permanent scarring that destroys follicles entirely.
Who gets it? TA disproportionately affects Black and South Asian women, where braids, locs, cornrows, weaves, and extensions are common styling practices. Athletes are also at risk: gymnasts and ballet dancers from tight buns, swimmers from repeated headgear friction. Men who wear tight man-buns or tight cornrows can develop it too, though less commonly.
Common hairstyle causes:
- Tight braids, locs, and cornrows
- High-tension weaves and hair extensions — especially glued or sewn close to the hairline
- Tight ponytails and buns worn daily at the same position
- Headgear that creates sustained friction or tension at the hairline
Where it appears: TA typically affects the frontal and temporal hairline — the margins where tension from a pulled-back style is greatest. A classic presenting sign is the fringe sign: a thin line of very fine, short hairs preserved along the very edge of the hairline, surrounded by recession behind it.
What it is not: TA can be confused with female-pattern hair loss (which causes vertex thinning, not hairline recession) or alopecia areata (patchy loss with no tension trigger). A dermatologist can distinguish these — usually with dermoscopy.
Early Warning Signs — What to Look For
Most patient-facing content on traction alopecia doesn’t teach people to self-check. These are the specific clinical signs to look for at your hairline:
Early traction alopecia appears as redness or small bumps at the hairline — signs that follicles are inflamed but not yet permanently damaged. Acting at this stage (hairstyle change) is when recovery is most reliable.
Perifollicular erythema: Redness or a pinkish tint around individual hair follicles at the hairline — often the earliest visible sign of active follicular inflammation.
Perifollicular papules: Small bumps or pimple-like lesions along the hairline margin, particularly at the points where your style applies the most tension. These signal active inflammation at the follicle level.
Fine broken hairs: Short, broken hair shafts at the temples or hairline — physically broken by tension, not shed from the root. This is different from normal daily shedding.
Hair thinning at the temples: The most characteristic early presentation. Thinning appears first at the frontotemporal hairline, not the crown.
Scalp soreness or tenderness: Pain or tightness at the hairline during or after applying a style. This is commonly dismissed as normal. It is not. Scalp tenderness after styling is a warning signal.
The fringe sign: A thin strip of fine, preserved hairs along the very edge of the hairline, with recession behind it — a pattern distinctive to traction alopecia.
What these signs mean: Perifollicular erythema and papules indicate active inflammation — this is the non-scarring stage, still reversible. If you are seeing these signs, remove the tension. Do not wait.
Non-Scarring vs. Scarring — The Critical Distinction
Non-scarring (early stage): Follicles are inflamed but structurally intact. Clinical signs include perifollicular erythema, papules, and the fringe sign. Reversibility is high. Removing the hairstyle tension allows follicles to recover.
Scarring (late stage): Follicles have been permanently replaced by fibrous tissue. Hair cannot regrow from a scarred follicle. On dermoscopy, clinicians identify this by the absence of follicular openings — replaced by smooth scar tissue. Reversibility is zero without surgical intervention.
How to tell which stage you are in: You can identify early warning signs yourself, but determining whether follicles are still viable requires dermoscopic assessment by a dermatologist. Do not attempt to self-diagnose scarring, and do not assume permanent damage just because hair loss is visible.
The key message: The vast majority of people researching traction alopecia online are in the early-stage or pre-clinical phase. Commercial clinic content disproportionately emphasises permanent scarring to drive consultation bookings. The honest picture is that late-stage irreversible traction alopecia takes years of persistent, unaddressed tension to develop. Most people reading this have time to act.
Reversibility Timeline — Does Traction Alopecia Grow Back?
This is the most important question for most people searching for this topic. Most online content either buries the answer or frames it around transplant consultations. Here is the direct answer.
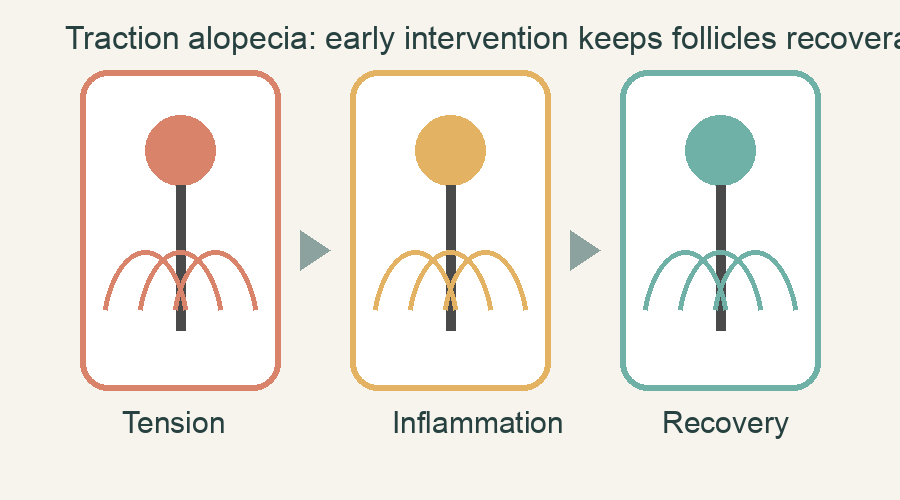
Most people who catch traction alopecia early — before scarring occurs — can expect full recovery with hairstyle modification. The window for reversal is open for the majority of people reading this. See a dermatologist to confirm your stage.
Early-stage (non-scarring) — reversibility is high:
- Initial reduction in shedding and inflammation after hairstyle change: 2–4 weeks
- Visible regrowth: 3–6 months (aligned with the normal hair growth cycle, which takes time to restart after follicular recovery)
- Full recovery to baseline hair density: 6–12 months in most cases
- Timeline caveat: Depends on how long tension was applied and the degree of follicular inflammation at the time of change. Longer-standing traction generally means a longer recovery window — but recovery is still expected for non-scarring cases.
Late-stage (scarring) — no natural recovery:
- Once follicles are replaced by fibrous tissue, no medical treatment restores them
- Hair transplantation is the only option to restore hair in a scarred recipient site
- This stage takes years of persistent, unaddressed traction to reach — it is the outcome of chronic neglect, not short-term styling
The Prevention Protocol — Hairstyle Guidance
The goal is not to abandon your hairstyle. It is to reduce tension at the hairline specifically. These recommendations are based on clinical evidence:
Rotation: Alternate tight styles with looser styles and give your hairline regular rest periods. Even a few days of low-tension styling between installs can reduce cumulative follicle stress.
Braids and locs: Install at medium tension — not maximum. Freshly installed braids should not cause scalp pain. Avoid gathering all hair to a single, high-tension attachment point.
Weaves and extensions: Avoid glued or sewn extensions attached directly at the hairline. Clip-in or tape-in extensions installed with minimal hairline tension are safer options. If you feel tightness or pulling at the hairline after installation, it needs to be loosened before you leave the salon.
Ponytails and buns: Vary the position — the same tight ponytail at the same location every day concentrates tension on the same follicles repeatedly. Use fabric ties or scrunchies rather than tight elastic bands.
Pain is a diagnostic signal: If a style causes scalp soreness or tenderness at the hairline, it is too tight. Loosen or remove it promptly. This principle applies regardless of style type.
Protective styles: Braids, locs, and cornrows can be worn without causing traction alopecia. The determining variable is tension level at installation and maintenance, not the style category. The goal is low-tension installation at the hairline margin — not style abandonment.
What Treatments Actually Help?
Hairstyle change
The treatment with the strongest and most consistent clinical support. In non-scarring traction alopecia, removing the cause is nearly always sufficient for full recovery. There is no pharmacological substitute for this step.
Topical minoxidil
Frequently recommended as an adjunct by clinics and GPs — but the evidence is weaker than most sources acknowledge. A systematic review of topical minoxidil for non-scarring alopecia found insufficient RCT evidence to support it as a standard treatment specifically for traction alopecia (Sung CT et al., J Drugs Dermatol 2019; PMID 30794366). The broader evidence base for TA remains small — predominantly case series and observational reports, not controlled trials.
Some dermatologists recommend minoxidil as a supportive adjunct during recovery, particularly when regrowth is slow, on the basis that it may extend the anagen phase while follicles are recovering. But it is not established as effective for TA in the way it is for androgenetic alopecia.
If you are considering minoxidil, discuss it with a dermatologist rather than starting independently. See our overview of oral minoxidil for the broader evidence context.
Intralesional corticosteroid injections
For early-stage cases with active perifollicular inflammation, intralesional triamcinolone injections can reduce inflammation and halt progression. This is a specialist procedure — not self-administered — and requires clinical assessment to confirm appropriateness.
Low-level laser therapy (LLLT)
A 2025 broad review of light-based therapies across alopecia presentations (Vanaria RJ, Chaudry A, Nestor MS. J Cosmet Dermatol 2025;24(9):e70434; DOI: 10.1111/jocd.70434) found supportive signals for LLLT; direct evidence specific to traction alopecia is limited. The evidence remains early-stage — small cohorts, short follow-up periods. LLLT is a potentially useful adjunct but is not a standard clinical recommendation for TA. See our overview of laser hair therapy for context, and ask your dermatologist whether it is appropriate for your case.
Hair transplantation
Appropriate only for late-stage permanent scarring — when dermoscopy confirms follicles have been destroyed and natural regrowth is impossible. Hair transplantation is a last resort for irreversible cases, not a routine treatment for early-stage traction alopecia. PRP injection is another advanced option some dermatologists consider alongside surgical planning.
The commercial clinic content that positions transplantation as the expected endpoint for any traction alopecia case does not reflect the clinical evidence for early-stage presentations. Most people who act on early warning signs will never need a transplant.
Cultural Context and Protective Styles
Traction alopecia disproportionately affects Black women. Braids, locs, and cornrows are cultural and protective hairstyle practices with deep roots — not habits to simply stop. Generic advice to “avoid tight hairstyles” is both practically unhelpful and culturally insensitive in this context.
The clinical goal is tension reduction at the hairline margin, not style avoidance. Specialist dermatology literature on management in patients with textured hair specifically recommends hairline-tension reduction strategies over hairstyle abandonment.
What this looks like in practice:
- Request low-tension installation at the hairline margin specifically — many experienced stylists are trained to accommodate this
- Schedule rest periods between installs, even a week or two of loose styling
- Pay attention to scalp tenderness immediately after installation — this is clinically meaningful information
- Seek stylists trained in low-tension techniques; this is increasingly a recognised skill in professional hair care communities
The cultural dimension of this condition means that effective advice has to be specific and actionable — and respectful of the practices it is asking patients to modify, not abandon.
When to See a Dermatologist
If you have early warning signs: Get a dermatology assessment within a few weeks. This is not emergency care, but it warrants prompt attention. Dermoscopic staging — confirming whether follicles are still viable — determines your management options.
Why a dermatologist specifically: A GP can identify visible hair loss, but may not be able to distinguish traction alopecia from CCCA (central centrifugal cicatricial alopecia), another scarring alopecia that disproportionately affects Black women and can present similarly. Dermoscopy is required to differentiate these. The distinction matters because management differs.
What to bring to the appointment:
- Photos of your typical hairstyle
- A rough timeline of when you began wearing that style and when you first noticed symptoms
Where to access care:
- UK: GP referral to NHS dermatology, or direct-access private dermatology
- US: Board-certified dermatologist; look for practices with a “hair disorders” subspecialty
If you want to understand what normal daily hair loss looks like as a baseline for comparison, see our guide to normal hair loss.
Frequently Asked Questions
Does traction alopecia grow back?
Yes — in most cases, if you catch it early and change your hairstyle. Early-stage traction alopecia damages but does not destroy the follicles. Once tension is removed, follicles can recover and hair regrows over 3–12 months. Late-stage traction alopecia, where follicles have been permanently replaced by scar tissue, cannot regrow without surgical intervention. Most people who identify the condition at the early-warning-sign stage will never reach permanent scarring.
How long does it take for traction alopecia to reverse?
For early-stage (non-scarring) cases: initial shedding reduction within 2–4 weeks of hairstyle change; visible regrowth in 3–6 months; full recovery to baseline density in most cases within 6–12 months. The timeline lengthens for cases where tension was applied over many years before the hairstyle change.
Is traction alopecia permanent?
Not if caught early. It becomes permanent only after follicles are destroyed by long-term scarring — a process that takes years of persistent, unaddressed traction. The vast majority of people who identify traction alopecia at the early-warning-sign stage are not in the permanent category.
Does minoxidil work for traction alopecia?
The evidence is weak. A systematic review of topical minoxidil for non-scarring alopecia (Sung CT et al., J Drugs Dermatol 2019; PMID 30794366) found insufficient RCT evidence to support it as a standard treatment for traction alopecia specifically. Hairstyle change is the primary and most supported treatment. Some dermatologists suggest minoxidil as an adjunct during recovery — discuss with your dermatologist whether it is appropriate for your situation.
What hairstyles are safe with traction alopecia?
Loose styles with varied positioning are safest during active recovery. Once recovered, protective styles installed at low tension are generally safe. The key variables are tension level at the hairline and the frequency of tight styling — not the style category itself.
Can I still wear braids or locs if I have traction alopecia?
Yes — with low-tension installation and regular rest periods for your hairline. The clinical recommendation is tension reduction, not style abandonment. Braids, locs, and cornrows installed at appropriate tension do not cause traction alopecia.
Conclusion
Traction alopecia is preventable and — in the vast majority of cases — reversible. The most important message: if you catch it early, changing your hairstyle is the treatment. You don’t need a transplant consultation. You don’t need to abandon your cultural hairstyle practices. You need to reduce tension at the hairline, pay attention to the signals your scalp is sending, and give your follicles 6–12 months to recover.
See a dermatologist to confirm your staging. Modify your hairstyle. Be consistent. Most people who act on early warning signs will recover fully. The window is still open for most people reading this — and the commercial clinic content designed to tell you otherwise has a financial reason to say so.