If you’re considering testosterone replacement therapy — or you’ve recently started it and noticed more hair in the shower drain — you want an honest answer, not a sales pitch.
Here it is: TRT can accelerate hair loss in men who are genetically susceptible to androgenetic alopecia (AGA). The mechanism is well-understood, the risk is real, and it depends heavily on your genetics and which formulation you’re using. At the same time, many men on TRT notice no significant additional hair loss at all.
This article explains the biology, what the evidence actually says about risk, how formulation choices affect DHT levels, and what mitigation options exist — all in terms you can bring to a conversation with your prescribing doctor or a dermatologist.
How TRT affects your hair: the DHT pathway
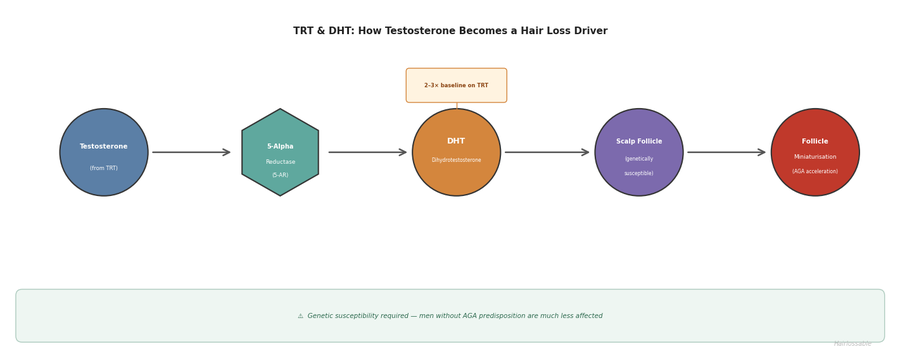
Testosterone doesn’t damage hair follicles directly. The culprit is dihydrotestosterone (DHT), a more potent androgen that testosterone converts into through an enzyme called 5-alpha reductase (5-AR).
When you introduce exogenous testosterone via TRT, your body has more raw material to convert. Depending on the formulation and dose, TRT typically elevates serum DHT by 2–3 times above your pre-treatment baseline.
In follicles that are genetically sensitive to androgens — specifically those in the frontal scalp and crown — DHT binds to androgen receptors and triggers a process called miniaturisation. Over time, affected follicles produce progressively thinner, shorter hairs until they stop producing a visible hair altogether. This is the same underlying process behind male pattern hair loss (androgenetic alopecia) in men who never touch TRT. TRT doesn’t create a new disease; it can accelerate one that was already written into your genetics.
The essential variable is genetics. Men with high androgen receptor sensitivity in scalp follicles, or with particular variants of the 5-alpha reductase enzyme, are at substantially higher risk of TRT-accelerated hair loss. Men without strong genetic susceptibility to AGA are much less likely to notice a difference.
Why only some men lose hair on TRT
Not everyone starting TRT will lose hair at an accelerated rate. The determining factors are:
Genetic predisposition to AGA. If you already have early signs of a receding hairline or crown thinning, your follicles are already responding to DHT. Raising DHT further via TRT will likely speed up that progression. If you have no family history of significant hair loss and no early signs in your own hairline, your follicles may be less sensitive to the elevated DHT.
Androgen receptor sensitivity. This is partly genetic and partially mediated by the AR gene on the X chromosome (inherited from your mother’s side). Men with higher androgen receptor density or sensitivity in scalp follicles are more vulnerable.
Baseline DHT and testosterone levels. Some men start TRT from a low baseline, meaning TRT brings their DHT to a normal or moderately elevated range. Others may push well above physiological norms depending on dose. Higher absolute DHT levels carry higher hair risk.
Age and existing AGA stage. AGA progresses with age regardless of TRT. Starting TRT in your 40s or 50s when some miniaturisation has already occurred is different from starting at 25 with a full, dense hairline.
The honest framing: TRT does not cause hair loss in men who have no genetic susceptibility to AGA. It accelerates a process that genetics has already enabled.
Does the TRT formulation matter for hair loss?
Yes — and this is one of the most clinically useful things to understand.
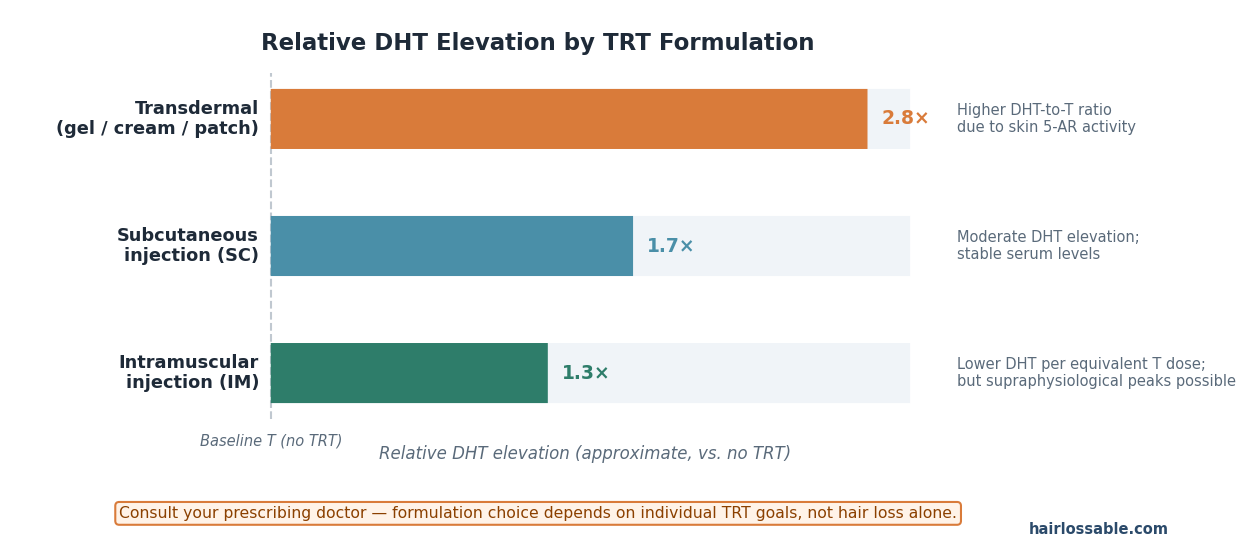
Transdermal testosterone (gels, patches, creams) produces higher DHT elevation relative to the testosterone dose. This is because transdermal application exposes the testosterone to significant 5-alpha reductase activity in the skin — particularly in skin cells of the scrotal area (for scrotal creams) and the general dermis. A 2014 systematic review and meta-analysis found transdermal TRT elevated serum DHT approximately 5.5-fold above baseline, compared to approximately 2.2-fold for intramuscular administration — a clinically meaningful difference.
Intramuscular injections (testosterone cypionate or enanthate) tend to produce lower DHT elevation per equivalent testosterone dose because the testosterone enters the bloodstream directly, bypassing the heavy 5-AR activity in skin. The DHT-to-testosterone ratio is generally lower with IM injections than with transdermal delivery.
Subcutaneous injections sit between transdermal and IM in terms of DHT conversion, though the data is less extensive.
Testosterone pellets (subdermal implants) have variable data, but DHT conversion tends to be moderate.
In practical terms: if hair preservation is a concern, intramuscular injections typically carry a more favourable DHT profile than gels or creams. This is a conversation worth having with your prescriber — formulation choice is a legitimate clinical consideration, not a fringe concern.
What does the evidence say about actual risk?
Quantifying risk is genuinely difficult here because studies vary in methodology, patient selection, and how “noticeable hair loss” is defined.
A 2025 clinical commentary from Baylor College of Medicine (urologist Dr. Blair Stocks and dermatologist Dr. Oyetewa Asempa) noted that roughly 40% of men on TRT observe noticeable shedding or accelerated loss within a year of starting. Other analyses report more conservative figures, and the evidence on absolute rates is mixed; study methodology varies considerably, but the directional finding — that TRT users with genetic susceptibility report higher rates of significant hair loss than non-TRT men — is consistent across sources.
The wide range reflects several real confounders: men who already had AGA and started TRT experience faster progression that gets attributed to TRT; men with no genetic susceptibility are unlikely to notice a difference; the dose, formulation, and duration of treatment all matter; and people who experience hair loss are more likely to report it than those who don’t.
The honest summary: TRT probably does increase hair loss risk in genetically susceptible men — the mechanism is clear and the evidence directionally consistent — but the absolute risk is not “most men will go bald faster.” The risk is most pronounced in men who already show signs of AGA or have strong family history on both sides.
Mitigation options to discuss with your doctor
If you’re concerned about hair loss on TRT, several evidence-based approaches exist. None of these should be started, adjusted, or stopped without discussion with your prescribing doctor or a dermatologist — especially since some interact with TRT directly and some carry their own side effect profiles.
Finasteride (1 mg daily)
Finasteride blocks the type 2 isoform of 5-alpha reductase, reducing serum DHT by approximately 65–70% while leaving testosterone levels intact or even slightly elevated. In men on TRT, adding finasteride has shown additive benefit for hair preservation compared to finasteride alone in several studies — because it’s specifically counteracting the TRT-driven DHT elevation.
Finasteride is FDA-approved for male pattern hair loss and has decades of data behind it. Side effects (reduced libido, erectile dysfunction, mood changes) occur in a minority of men and are typically reversible on discontinuation, though a subset of men report persistent effects. This is a trade-off only you and your doctor can weigh.
Dutasteride (0.5 mg daily)
Dutasteride inhibits both type 1 and type 2 isoforms of 5-alpha reductase, achieving approximately 99% DHT suppression — significantly more complete than finasteride. It is approved for benign prostatic hyperplasia and is used off-label for hair loss. For men on TRT with high genetic susceptibility to AGA, the more complete DHT suppression can be clinically meaningful.
The more comprehensive DHT suppression also means more complete removal of DHT’s non-hair physiological effects, which some men find affects libido or mood more than finasteride. Again — a prescriber conversation, not a self-titration decision.
Topical finasteride
Topical finasteride applied to the scalp achieves localised DHT suppression at the follicle level with substantially lower systemic absorption than oral finasteride. This is used by some TRT patients who want to minimise DHT’s effect on scalp follicles while reducing the risk of systemic side effects.
Evidence for topical finasteride in AGA is solid, and its use alongside TRT is growing — particularly among men who’ve had side effects on oral finasteride or who want to keep systemic DHT suppression minimal while protecting scalp follicles.
Formulation switch
As described above, switching from a transdermal formulation (gel, cream, patch) to intramuscular injections may reduce your DHT-to-testosterone ratio without changing your therapeutic testosterone outcome. This is the least invasive of the mitigation options because it doesn’t add another medication — it adjusts how your TRT is delivered.
Not all prescribers monitor DHT routinely; it’s reasonable to ask for a serum DHT measurement and discuss whether formulation is contributing to elevated DHT.
What doesn’t meaningfully help
DHT-blocking shampoos (ketoconazole, saw palmetto-based shampoos) may have a mild adjunctive role in reducing scalp DHT, but they have no meaningful evidence of providing significant protection in the context of TRT-elevated systemic DHT. They’re not a substitute for the options above.
If you’re already noticing hair loss on TRT
If you’ve been on TRT for some months and have started to notice accelerated thinning or recession, the first step is distinguishing TRT-accelerated AGA from other causes of hair loss (stress, nutritional deficiencies, thyroid dysfunction) that may coincide with starting TRT. A dermatologist can help with this assessment.
For TRT-accelerated AGA specifically, the mitigation options above remain relevant — adding DHT-blocking medication or switching formulation can slow or stabilise progression even after it has started. Early intervention matters: once follicles have fully miniaturised and become dormant (producing no visible hair), they are generally not recoverable with medical therapy. Acting before that stage is preferable.
Questions worth raising with your doctor if you’re noticing hair loss on TRT:
- What is my current serum DHT level, and is it significantly above the normal range?
- Would switching to IM injections reduce my DHT exposure?
- Is finasteride or dutasteride appropriate to consider given my overall health picture?
- Are there other treatable causes of my current shedding worth ruling out?
What TRT does not do
To be clear: TRT does not cause a different type of hair loss, does not damage follicles through a mechanism unrelated to DHT, and does not cause irreversible loss in men with no genetic susceptibility to AGA. The mechanism is entirely androgen-mediated, which means DHT-targeted interventions have genuine potential to protect hair on TRT.
TRT is also a medically legitimate, widely prescribed treatment for hypogonadism with documented benefits for quality of life, metabolic health, bone density, and mood in appropriately diagnosed men. The hair loss risk, while real for susceptible men, should be weighed against these benefits and managed — not used as grounds to avoid a treatment that may be clinically indicated for you.
The bottom line
- TRT raises DHT levels, typically 2–3× above baseline, which can accelerate androgenetic alopecia in genetically susceptible men.
- The key variable is genetics: if you have no strong predisposition to AGA, your hair risk from TRT is low.
- Formulation matters: transdermal delivery (gels, creams) produces substantially higher DHT elevation than intramuscular injections.
- Evidence-based mitigation options exist — finasteride, dutasteride, topical finasteride, and formulation switching — all of which should be discussed with your prescribing doctor, not self-initiated.
- Many men on TRT do not experience significant additional hair loss; the risk is real but is neither universal nor inevitable.
If hair loss is a significant concern for you personally, raise it explicitly with your prescriber before starting TRT, or with a dermatologist if you’ve already started. It’s a solvable problem for most men — but it requires a prescriber in the conversation.
Sources and further reading
- Stocks B, Asempa O. “Does testosterone replacement therapy cause hair loss?” Baylor College of Medicine Blog Network. 11 August 2025. https://blogs.bcm.edu/2025/08/11/does-testosterone-replacement-therapy-cause-hair-loss/ — clinical commentary on TRT and androgenetic alopecia risk by named BCM physicians (urologist + dermatologist); source of the ~40% shedding figure
- Borst SE, Shuster JJ, Zou B, Ye F, Jia H, Wokhlu A, Yarrow JF. “Cardiovascular risks and elevation of serum DHT vary by route of testosterone administration: a systematic review and meta-analysis.” BMC Medicine. 2014;12:211. doi:10.1186/s12916-014-0211-5. https://pmc.ncbi.nlm.nih.gov/articles/PMC4245724/ — formulation-specific DHT elevation data; transdermal TRT elevated DHT ~5.5-fold vs ~2.2-fold for intramuscular
- Kaufman KD — finasteride in men with AGA; mechanism and efficacy data
- Clark RV et al. — dutasteride and dual 5-alpha reductase inhibition; DHT suppression data
- Related Hairlossable topics to add once live: DHT and hair loss, finasteride for hair loss, finasteride side effects, dutasteride for hair loss, topical finasteride, and male pattern hair loss.